Evaluation of decision support to wean patients from mechanical ventilation in intensive care: a prospective study reporting clinical and physiological outcomes.
Marcela P Vizcaychipi, Dan S Karbing, Laura Martins, Amandeep Gupta, Jeronimo Moreno-Cuesta, Manu Naik, Ingeborg Welters, Suveer Singh, Georgina Randell, Leyla Osman, Stephen E Rees
{"title":"Evaluation of decision support to wean patients from mechanical ventilation in intensive care: a prospective study reporting clinical and physiological outcomes.","authors":"Marcela P Vizcaychipi, Dan S Karbing, Laura Martins, Amandeep Gupta, Jeronimo Moreno-Cuesta, Manu Naik, Ingeborg Welters, Suveer Singh, Georgina Randell, Leyla Osman, Stephen E Rees","doi":"10.1007/s10877-024-01231-5","DOIUrl":null,"url":null,"abstract":"<p><p>This study investigated the clinical and physiological response to use of the BEACON Caresystem, a bedside open-loop decision support system providing advice to guide clinicians when weaning patients from invasive mechanical ventilation. Multicenter prospective study conducted in five adult intensive care units in the UK. Following screening and assent, intubated patients mechanically ventilated for > 24 h were randomized to intervention or usual care. Intervention consisted of application of the BEACON Caresystem's advice on tidal volume/inspiratory pressure, inspired oxygen, respiratory rate and PEEP. Usual care was defined as local clinical practice. The primary outcome was duration of mechanical ventilation. Secondary outcomes quantified prolonged intubation and survival; adverse events; ventilator settings and physiological state; time spent in ventilator modes; links to other therapy; the frequency of advice utilization and time spent outside normal physiological limits. The study was terminated early with a total of 112 patients included. Fifty-four were randomised to the intervention arm and fifty-eight to usual care. The study was underpowered and no significant differences were seen in duration of mechanical ventilation (p = 0.773), prolonged intubation or survival. Intervention arm patients had lower rates of adverse events (p = 0.016), including fewer hypoxaemic events (p = 0.008) and lower values of PEEP (p = 0.030) and tidal volume (p = 0.042). Values of peak inspiratory pressure and pressure support were reduced but at the boarder of statistical significance (p = 0.104, p = 0.093, respectively). No differences were seen for time in ventilator mode or other therapy. Advice presented by the decision support system was applied at the beside an average of 88% of occasions, with a significantly increased number of changes only in inspired oxygen fraction. No significant differences were seen in time spent outside physiological limits. This study investigated the use of the BEACON Caresystem, an open loop clinical decision support system providing advice on ventilator settings. It was terminated early, with no significant difference shown in duration of mechanical ventilation, the primary outcome. Application of advice indicated potential for fewer adverse events and improved physiological status. (Trial registration ClinicalTrials.gov under NCT03249623. Registered 22nd June 2017).</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"393-404"},"PeriodicalIF":2.2000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12049327/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-024-01231-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/9 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
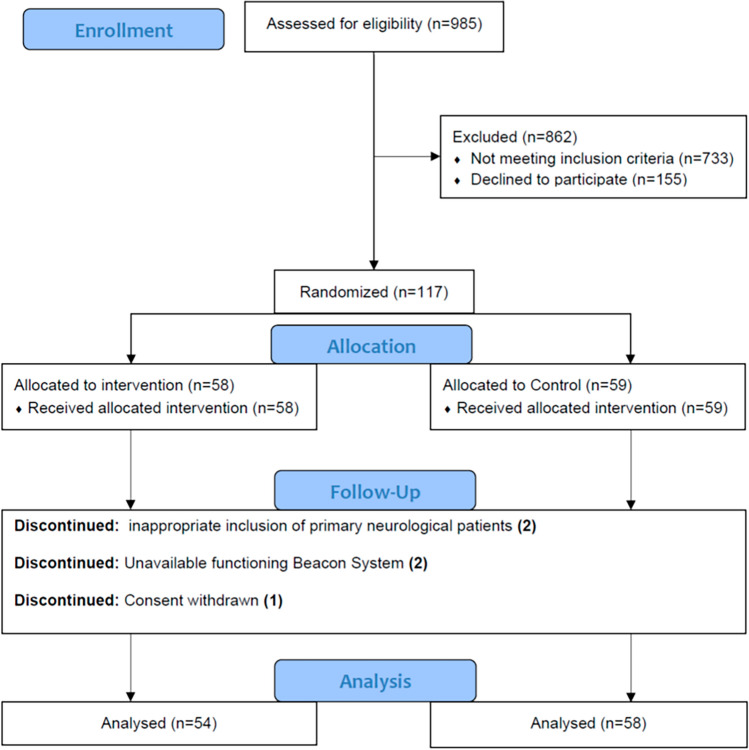
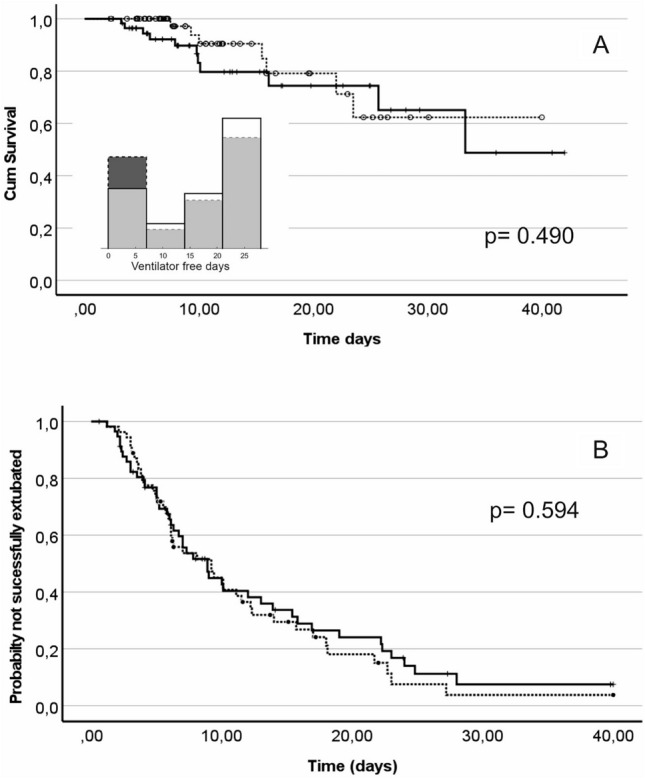
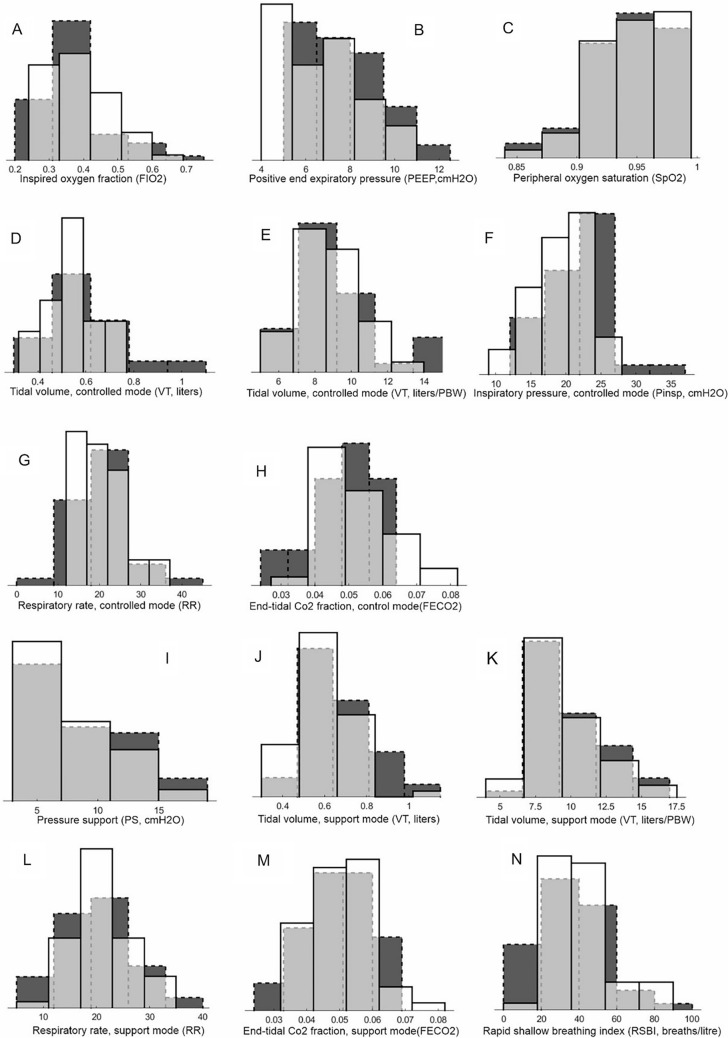
This study investigated the clinical and physiological response to use of the BEACON Caresystem, a bedside open-loop decision support system providing advice to guide clinicians when weaning patients from invasive mechanical ventilation. Multicenter prospective study conducted in five adult intensive care units in the UK. Following screening and assent, intubated patients mechanically ventilated for > 24 h were randomized to intervention or usual care. Intervention consisted of application of the BEACON Caresystem's advice on tidal volume/inspiratory pressure, inspired oxygen, respiratory rate and PEEP. Usual care was defined as local clinical practice. The primary outcome was duration of mechanical ventilation. Secondary outcomes quantified prolonged intubation and survival; adverse events; ventilator settings and physiological state; time spent in ventilator modes; links to other therapy; the frequency of advice utilization and time spent outside normal physiological limits. The study was terminated early with a total of 112 patients included. Fifty-four were randomised to the intervention arm and fifty-eight to usual care. The study was underpowered and no significant differences were seen in duration of mechanical ventilation (p = 0.773), prolonged intubation or survival. Intervention arm patients had lower rates of adverse events (p = 0.016), including fewer hypoxaemic events (p = 0.008) and lower values of PEEP (p = 0.030) and tidal volume (p = 0.042). Values of peak inspiratory pressure and pressure support were reduced but at the boarder of statistical significance (p = 0.104, p = 0.093, respectively). No differences were seen for time in ventilator mode or other therapy. Advice presented by the decision support system was applied at the beside an average of 88% of occasions, with a significantly increased number of changes only in inspired oxygen fraction. No significant differences were seen in time spent outside physiological limits. This study investigated the use of the BEACON Caresystem, an open loop clinical decision support system providing advice on ventilator settings. It was terminated early, with no significant difference shown in duration of mechanical ventilation, the primary outcome. Application of advice indicated potential for fewer adverse events and improved physiological status. (Trial registration ClinicalTrials.gov under NCT03249623. Registered 22nd June 2017).
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
