{"title":"Polysomnographic features of children with obesity: body mass index predict severe obstructive sleep apnea in obese children?","authors":"Rungrat Sukharom, Prakarn Tovichien, Kanokporn Udomittipong, Pinyapach Tiamduangtawan, Wattanachai Chotinaiwattarakul","doi":"10.3345/cep.2024.00066","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Few studies have explored the polysomnographic features of children with obesity.</p><p><strong>Purpose: </strong>This study aimed to explore the demographic and polysomnographic features of obese children and determine whether body mass index (BMI) could predict severe obstructive sleep apnea (OSA).</p><p><strong>Methods: </strong>This cross-sectional study recruited obese children who underwent diagnostic polysomnography between January 2019 and March 2022. We explored demographic and anthropometric measures as well as polysomnographic abnormalities among them. We used receiver operating characteristic curves and logistic regression analyses to determine the optimal cutoff values of anthropometric variables for predicting severe OSA.</p><p><strong>Results: </strong>A total of 132 children with obesity (76.5% male; mean age, 12.5±3.2 years) were included. Severe OSA was identified in 64 children (48.5%). Desaturation was observed in 59.8%, while 23.5% had hyperarousal, 20.5% had sleep-related hypoventilation, 60.6% had positional OSA, 40.2% had rapid eye movement-related OSA, and 5.0% had obesity hypoventilation syndrome. Among them, BMI (odds ratio [OR], 1.11; 95% confidence interval [CI], 1.05-1.17; P<0.001), neck circumference (OR, 1.15; 95% CI, 1.07-1.25; P<0.001), and waist circumference (OR, 1.04; 95% CI, 1.02- 1.07; P=0.001) were significantly associated with severe OSA. These findings suggest a cutoff BMI for predicting severe OSA of greater than 29.2 kg/m2 with 81.3% sensitivity and 48.5% specificity.</p><p><strong>Conclusion: </strong>Severe OSA is common in children with obesity; thus, we recommend screening children with obesity and a BMI greater than 29.2 kg/m2 for severe OSA.</p>","PeriodicalId":36018,"journal":{"name":"Clinical and Experimental Pediatrics","volume":" ","pages":"80-90"},"PeriodicalIF":3.6000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11725614/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3345/cep.2024.00066","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/6 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Few studies have explored the polysomnographic features of children with obesity.
Purpose: This study aimed to explore the demographic and polysomnographic features of obese children and determine whether body mass index (BMI) could predict severe obstructive sleep apnea (OSA).
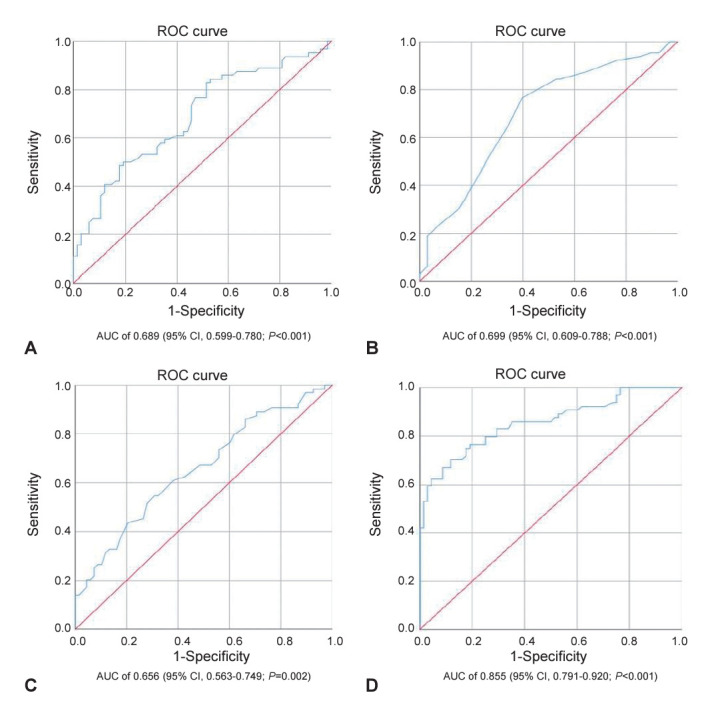
Methods: This cross-sectional study recruited obese children who underwent diagnostic polysomnography between January 2019 and March 2022. We explored demographic and anthropometric measures as well as polysomnographic abnormalities among them. We used receiver operating characteristic curves and logistic regression analyses to determine the optimal cutoff values of anthropometric variables for predicting severe OSA.
Results: A total of 132 children with obesity (76.5% male; mean age, 12.5±3.2 years) were included. Severe OSA was identified in 64 children (48.5%). Desaturation was observed in 59.8%, while 23.5% had hyperarousal, 20.5% had sleep-related hypoventilation, 60.6% had positional OSA, 40.2% had rapid eye movement-related OSA, and 5.0% had obesity hypoventilation syndrome. Among them, BMI (odds ratio [OR], 1.11; 95% confidence interval [CI], 1.05-1.17; P<0.001), neck circumference (OR, 1.15; 95% CI, 1.07-1.25; P<0.001), and waist circumference (OR, 1.04; 95% CI, 1.02- 1.07; P=0.001) were significantly associated with severe OSA. These findings suggest a cutoff BMI for predicting severe OSA of greater than 29.2 kg/m2 with 81.3% sensitivity and 48.5% specificity.
Conclusion: Severe OSA is common in children with obesity; thus, we recommend screening children with obesity and a BMI greater than 29.2 kg/m2 for severe OSA.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
