{"title":"Calcineurin-Inhibitor Discontinuation Could Reduce the Risk of De Novo Malignancies After Liver Transplantation for Alcohol-Related Liver Disease","authors":"Domitille Erard, Anouk Steiner, Olivier Boillot, Elsa Thimonier, Mélanie Vallin, Florian Veyre, Olivier Guillaud, Sylvie Radenne, Jérôme Dumortier","doi":"10.1111/ctr.70014","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>De novo malignancies are one of the leading causes of death after liver transplantation (LT), particularly in patients transplanted for alcohol-related liver disease (ALD). This retrospective study aimed to assess risk factors for malignancies and to evaluate the impact of calcineurin inhibitor (CNI) discontinuation.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>From 1990 to 2015, all patients transplanted for ALD were included.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 493 patients were included, 77.9% were male and the median age at LT was 54 years. After LT, 278 de novo malignancies were diagnosed in 214 patients (43.4%). The cumulative incidence of de novo malignancies was 16.3% at 5 years, 34.4% at 10 years, and 49.8% at 15 years. In multivariate analysis, the independent risk factors were male gender (HR = 1.6), and active or weaned smoking (HR = 2.0). Discontinuation of CNI was a protective factor (HR = 0.6). Survival after diagnosis of de novo malignancy was 42.7% at 5 years and 27.5% at 10 years.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Our results confirm the major incidence of de novo malignancies after LT for ALD, as well as the important role of non-modifiable risk factors such as smoking and gender. CNI discontinuation is a protective factor, and the only adaptable, and could be proposed in smoker male patients transplanted for ALD.</p>\n </section>\n </div>","PeriodicalId":10467,"journal":{"name":"Clinical Transplantation","volume":"38 11","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-11-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.70014","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Transplantation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ctr.70014","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
De novo malignancies are one of the leading causes of death after liver transplantation (LT), particularly in patients transplanted for alcohol-related liver disease (ALD). This retrospective study aimed to assess risk factors for malignancies and to evaluate the impact of calcineurin inhibitor (CNI) discontinuation.
Methods
From 1990 to 2015, all patients transplanted for ALD were included.
Results
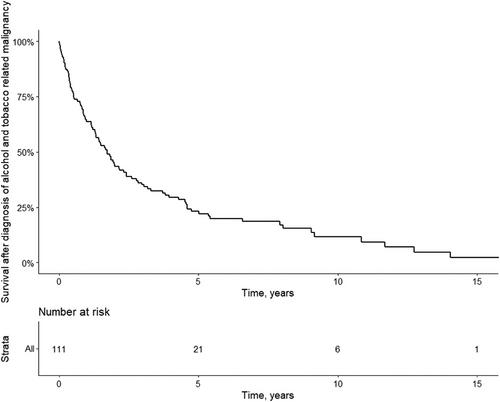
A total of 493 patients were included, 77.9% were male and the median age at LT was 54 years. After LT, 278 de novo malignancies were diagnosed in 214 patients (43.4%). The cumulative incidence of de novo malignancies was 16.3% at 5 years, 34.4% at 10 years, and 49.8% at 15 years. In multivariate analysis, the independent risk factors were male gender (HR = 1.6), and active or weaned smoking (HR = 2.0). Discontinuation of CNI was a protective factor (HR = 0.6). Survival after diagnosis of de novo malignancy was 42.7% at 5 years and 27.5% at 10 years.
Conclusion
Our results confirm the major incidence of de novo malignancies after LT for ALD, as well as the important role of non-modifiable risk factors such as smoking and gender. CNI discontinuation is a protective factor, and the only adaptable, and could be proposed in smoker male patients transplanted for ALD.
期刊介绍:
Clinical Transplantation: The Journal of Clinical and Translational Research aims to serve as a channel of rapid communication for all those involved in the care of patients who require, or have had, organ or tissue transplants, including: kidney, intestine, liver, pancreas, islets, heart, heart valves, lung, bone marrow, cornea, skin, bone, and cartilage, viable or stored.
Published monthly, Clinical Transplantation’s scope is focused on the complete spectrum of present transplant therapies, as well as also those that are experimental or may become possible in future. Topics include:
Immunology and immunosuppression;
Patient preparation;
Social, ethical, and psychological issues;
Complications, short- and long-term results;
Artificial organs;
Donation and preservation of organ and tissue;
Translational studies;
Advances in tissue typing;
Updates on transplant pathology;.
Clinical and translational studies are particularly welcome, as well as focused reviews. Full-length papers and short communications are invited. Clinical reviews are encouraged, as well as seminal papers in basic science which might lead to immediate clinical application. Prominence is regularly given to the results of cooperative surveys conducted by the organ and tissue transplant registries.
Clinical Transplantation: The Journal of Clinical and Translational Research is essential reading for clinicians and researchers in the diverse field of transplantation: surgeons; clinical immunologists; cryobiologists; hematologists; gastroenterologists; hepatologists; pulmonologists; nephrologists; cardiologists; and endocrinologists. It will also be of interest to sociologists, psychologists, research workers, and to all health professionals whose combined efforts will improve the prognosis of transplant recipients.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
