Ning Zhou, Kui Zhang, Bokang Qiao, Cong Chen, Xiaobo Guo, Wei Fu, Jubing Zheng, Jie Du, Ran Dong
{"title":"Personalized risk prediction of mortality and rehospitalization for heart failure in patients undergoing mitral valve repair surgery.","authors":"Ning Zhou, Kui Zhang, Bokang Qiao, Cong Chen, Xiaobo Guo, Wei Fu, Jubing Zheng, Jie Du, Ran Dong","doi":"10.3389/fcvm.2024.1470987","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Accurately assessing the postoperative mortality and rehospitalization for heart failure risks in patients undergoing mitral valve repair surgery is of significant importance for individualized medical strategies.</p><p><strong>Objective: </strong>We sought to develop and validate a risk assessment system for the prediction of mortality and rehospitalization for heart failure.</p><p><strong>Methods: </strong>Personalized risk prediction system of mortality and rehospitalization for heart failure was developed. For developing a prediction system with death as the outcome, there were 965 patients (70%) and 413 patients (30%) were included in the the derivation cohort and the validation cohort. For developing a prediction system with rehospitalization for heart failure as the outcome, there were 927 patients (70%) and 398 patients (30%) were included in the derivation cohort and the validation cohort. There were 42 routine clinical variables used to develop the models. The performance evaluation of the model is based on the area under the curve (AUC). Evaluate the improvement with Euro Score II according to NRI and IDI net reclassification improvement (NRI) and integrated discrimination improvement (IDI).</p><p><strong>Results: </strong>The median follow-up time was 685 days, the incidence of death was 3.85% (<i>n</i> = 53), and the incidence of rehospitalization for heart failure was 10.01% (<i>n</i> = 138). The AUC values of the mortality prediction model in the derivation and validation cohorts were 0.825 (0.764-0.886) and 0.808 (0.699-0.917), respectively. The AUC values of the rehospitalization for heart failure prediction model in the derivation and validation cohorts were 0.794 (0.756-0.832) and 0.812 (0.758-0.866), respectively. NRI and IDI showed that the mortality prediction model exhibited superior performance than the Euro Score II. The mortality and rehospitalization for heart failure risk prediction models effectively stratified patients into different risk subgroups.</p><p><strong>Conclusion: </strong>The developed and validated models exhibit satisfactory performance in prediction of all-cause mortality and rehospitalization for heart failure after mitral valve repair surgery.</p><p><strong>Clinical trial registration: </strong>http://www.clinicaltrials.gov, Unique identifier: (NCT05141292).</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"11 ","pages":"1470987"},"PeriodicalIF":2.8000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11563966/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2024.1470987","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Accurately assessing the postoperative mortality and rehospitalization for heart failure risks in patients undergoing mitral valve repair surgery is of significant importance for individualized medical strategies.
Objective: We sought to develop and validate a risk assessment system for the prediction of mortality and rehospitalization for heart failure.
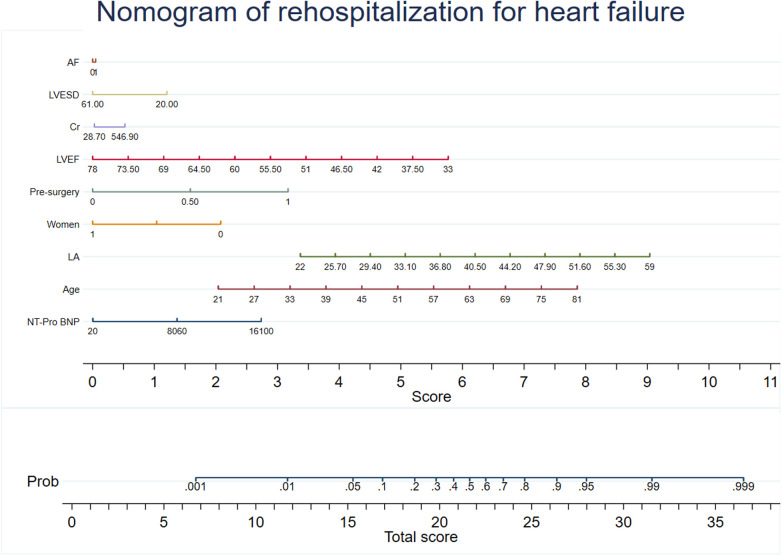
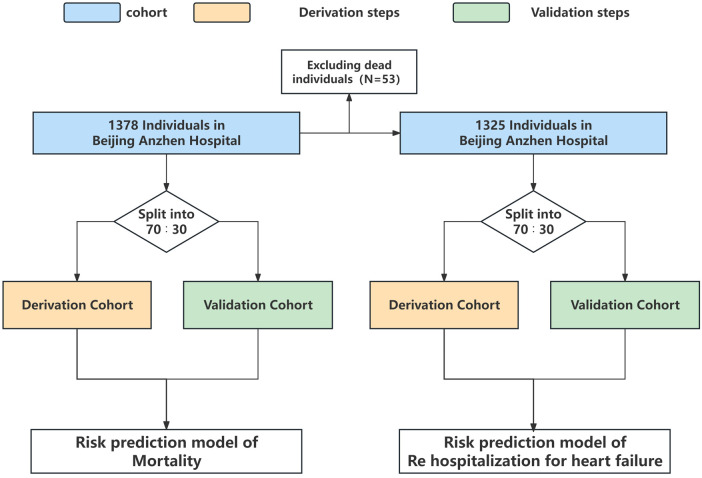
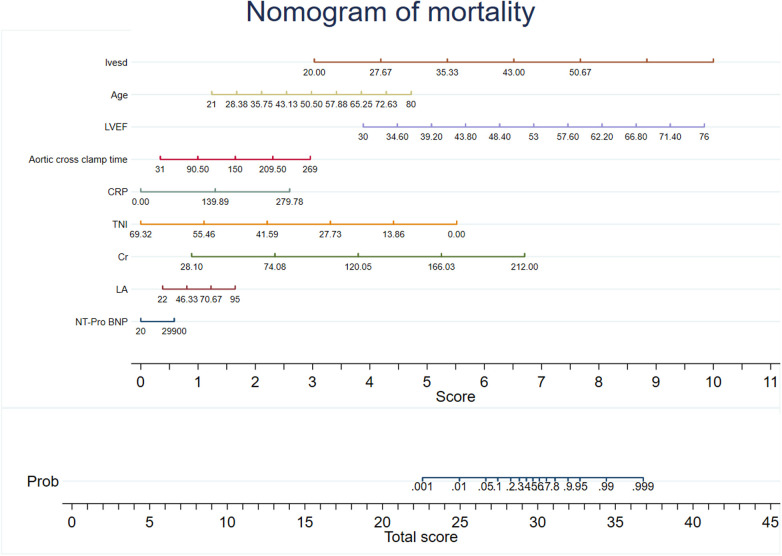
Methods: Personalized risk prediction system of mortality and rehospitalization for heart failure was developed. For developing a prediction system with death as the outcome, there were 965 patients (70%) and 413 patients (30%) were included in the the derivation cohort and the validation cohort. For developing a prediction system with rehospitalization for heart failure as the outcome, there were 927 patients (70%) and 398 patients (30%) were included in the derivation cohort and the validation cohort. There were 42 routine clinical variables used to develop the models. The performance evaluation of the model is based on the area under the curve (AUC). Evaluate the improvement with Euro Score II according to NRI and IDI net reclassification improvement (NRI) and integrated discrimination improvement (IDI).
Results: The median follow-up time was 685 days, the incidence of death was 3.85% (n = 53), and the incidence of rehospitalization for heart failure was 10.01% (n = 138). The AUC values of the mortality prediction model in the derivation and validation cohorts were 0.825 (0.764-0.886) and 0.808 (0.699-0.917), respectively. The AUC values of the rehospitalization for heart failure prediction model in the derivation and validation cohorts were 0.794 (0.756-0.832) and 0.812 (0.758-0.866), respectively. NRI and IDI showed that the mortality prediction model exhibited superior performance than the Euro Score II. The mortality and rehospitalization for heart failure risk prediction models effectively stratified patients into different risk subgroups.
Conclusion: The developed and validated models exhibit satisfactory performance in prediction of all-cause mortality and rehospitalization for heart failure after mitral valve repair surgery.
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
