{"title":"Opinions on Amblyopia Treatment in Microtropia - A Questionnaire Study of Orthoptists in Scandinavia.","authors":"Jannicke Røe, Gemma Arblaster","doi":"10.22599/bioj.316","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Microtropia is a small angle strabismus of less than or equal to ten prism diopters. It often co-exists with anisometropia, and patients may require amblyopia treatment. Diplopia following amblyopia treatment is considered rare, but older literature can advise caution when treating amblyopia in microtropia. This study aimed to explore orthoptists' opinions on amblyopia treatment in microtropia.</p><p><strong>Methods: </strong>Orthoptists working in Scandinavia were invited to complete an online questionnaire regarding their views on amblyopia treatment. They were presented with three different clinical scenarios: 1) patient with anisometropia; 2) patient with anisometropia and microtropia with identity; and 3) patient with anisometropia and microtropia without identity.</p><p><strong>Results: </strong>The questionnaire received responses from 30 orthoptists, which were analysed. The results showed a significantly higher concern for diplopia in patients with microtropia undergoing amblyopia treatment than in patients with anisometropia. They responded that to prevent diplopia, it is more important to stop amblyopia treatment before equal visual acuity (VA) is reached in microtropia compared to anisometropia. Thus, amblyopia treatment was stopped more often in microtropia, even if VA was improving and diplopia was absent. Equal VA was perceived to be more difficult to achieve in microtropia, both with and without identity, compared to anisometropia.</p><p><strong>Conclusion: </strong>Despite more recent evidence that diplopia following amblyopia treatment is extremely rare, orthoptists working in Scandinavia reported more concerns about diplopia when treating amblyopia in microtropia than in anisometropia. Stopping amblyopia treatment in microtropia before equal VA was achieved was considered somewhat important to prevent diplopia. Orthoptists also reported that equal VA was difficult to achieve in patients with microtropia, both with and without identity. Further research would help improve the evidence and inform clinical decisions about microtropia and amblyopia treatment in microtropia.</p>","PeriodicalId":36083,"journal":{"name":"British and Irish Orthoptic Journal","volume":"20 1","pages":"226-234"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11568811/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"British and Irish Orthoptic Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22599/bioj.316","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Microtropia is a small angle strabismus of less than or equal to ten prism diopters. It often co-exists with anisometropia, and patients may require amblyopia treatment. Diplopia following amblyopia treatment is considered rare, but older literature can advise caution when treating amblyopia in microtropia. This study aimed to explore orthoptists' opinions on amblyopia treatment in microtropia.
Methods: Orthoptists working in Scandinavia were invited to complete an online questionnaire regarding their views on amblyopia treatment. They were presented with three different clinical scenarios: 1) patient with anisometropia; 2) patient with anisometropia and microtropia with identity; and 3) patient with anisometropia and microtropia without identity.
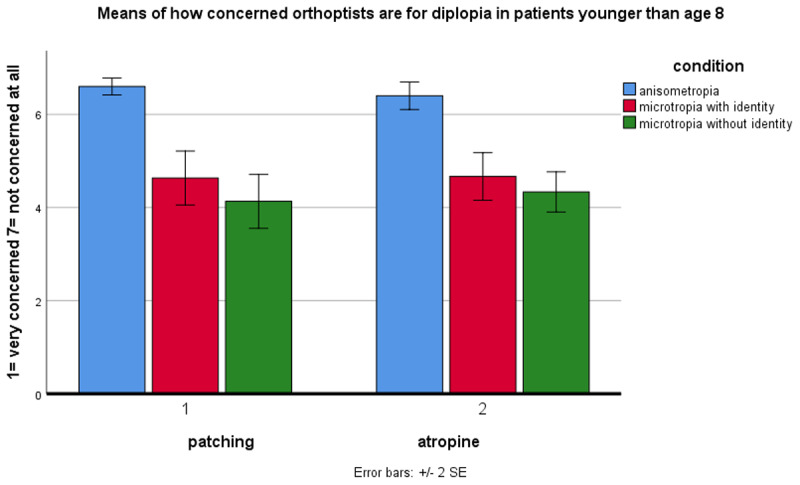
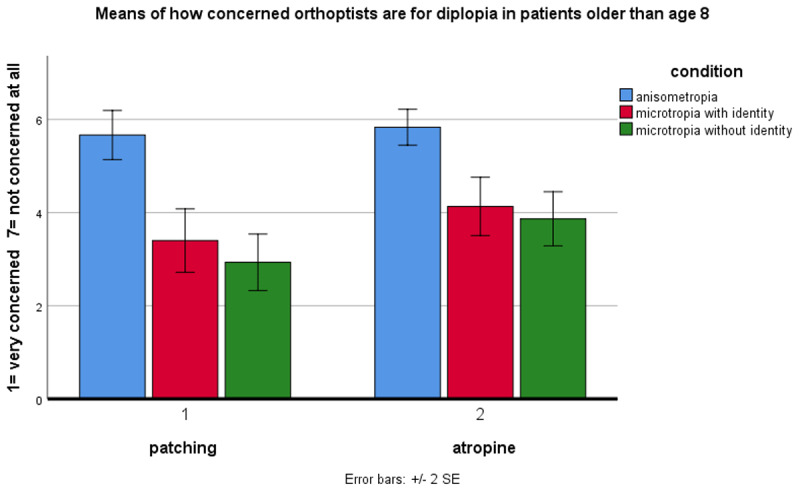
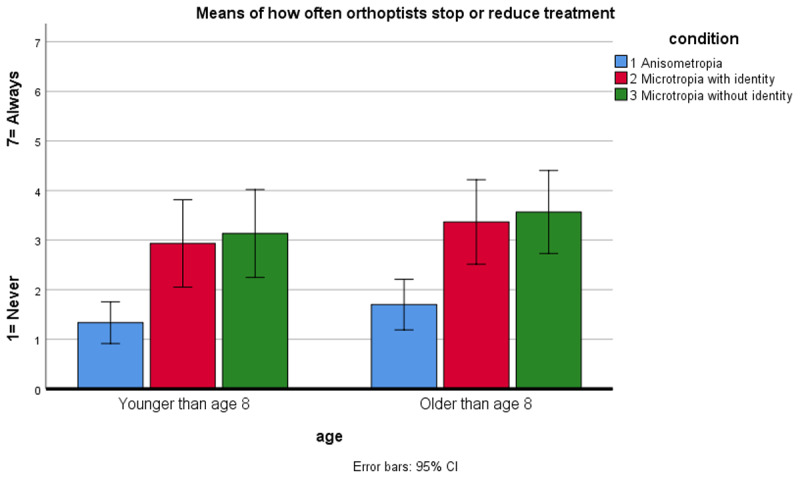
Results: The questionnaire received responses from 30 orthoptists, which were analysed. The results showed a significantly higher concern for diplopia in patients with microtropia undergoing amblyopia treatment than in patients with anisometropia. They responded that to prevent diplopia, it is more important to stop amblyopia treatment before equal visual acuity (VA) is reached in microtropia compared to anisometropia. Thus, amblyopia treatment was stopped more often in microtropia, even if VA was improving and diplopia was absent. Equal VA was perceived to be more difficult to achieve in microtropia, both with and without identity, compared to anisometropia.
Conclusion: Despite more recent evidence that diplopia following amblyopia treatment is extremely rare, orthoptists working in Scandinavia reported more concerns about diplopia when treating amblyopia in microtropia than in anisometropia. Stopping amblyopia treatment in microtropia before equal VA was achieved was considered somewhat important to prevent diplopia. Orthoptists also reported that equal VA was difficult to achieve in patients with microtropia, both with and without identity. Further research would help improve the evidence and inform clinical decisions about microtropia and amblyopia treatment in microtropia.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
