Veno-Venous Extracorporeal Membrane Oxygenation Support for Severe Primary Graft Dysfunction Is Associated With Reduced Airway Complications After Lung Transplantation
Kentaro Noda, Mohamed-Ali H. Jawad-Makki, Ernest G. Chan, John Ryan, Masashi Furukawa, Chadi A. Hage, Pablo G. Sanchez
{"title":"Veno-Venous Extracorporeal Membrane Oxygenation Support for Severe Primary Graft Dysfunction Is Associated With Reduced Airway Complications After Lung Transplantation","authors":"Kentaro Noda, Mohamed-Ali H. Jawad-Makki, Ernest G. Chan, John Ryan, Masashi Furukawa, Chadi A. Hage, Pablo G. Sanchez","doi":"10.1111/ctr.70029","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Early utilization of extracorporeal membrane oxygenation (ECMO) improves the clinical outcomes of patients with severe primary graft dysfunction (PGD3) after lung transplantation. Although there is a survival benefit, the impact of ECMO on airway complications has not been investigated. This study aims to describe the clinical association between posttransplant methods of support and the severity of acute airway anastomosis complications in patients with PGD3 following bilateral lung transplantation.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Data from adult bilateral lung transplant patients diagnosed with PGD3 at our institution were retrospectively reviewed. Bronchial anastomosis necrosis (ischemia reperfusion injury [IRI]) that developed within a month after transplantation was graded. The data were compared among the groups of veno-venous ECMO (VV-ECMO) (<i>n</i> = 77), veno-arterial ECMO (VA-ECMO) (<i>n</i> = 14), and mechanical ventilation (MV, <i>n</i> = 33).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Higher levels of support (VV/VA-ECMO) were associated with a lower incidence of PGD3, which was highest in recipients on MV only (<i>M</i><sup>2</sup> = 19.54, <i>r</i> = −0.41, <i>p</i> < 0.001). In a multivariable competing risk analysis, VV-ECMO was protective against chronic allograft dysfunction (CLAD) relative to the MV group (HR: 0.36 [0.13–0.96], <i>p</i> = 0.042). There was no relationship between posttransplant support and survival.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>This study suggests posttransplant VV-ECMO support in patients who develop PGD3 may confer a protective advantage over MV alone in the prevention of ischemic reperfusion injury. VV-ECMO was associated with lower IRI grades and lower rates of BOS after transplantation. Future studies investigating the causal mechanisms are warranted.</p>\n </section>\n </div>","PeriodicalId":10467,"journal":{"name":"Clinical Transplantation","volume":"38 11","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-11-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.70029","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Transplantation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ctr.70029","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Early utilization of extracorporeal membrane oxygenation (ECMO) improves the clinical outcomes of patients with severe primary graft dysfunction (PGD3) after lung transplantation. Although there is a survival benefit, the impact of ECMO on airway complications has not been investigated. This study aims to describe the clinical association between posttransplant methods of support and the severity of acute airway anastomosis complications in patients with PGD3 following bilateral lung transplantation.
Methods
Data from adult bilateral lung transplant patients diagnosed with PGD3 at our institution were retrospectively reviewed. Bronchial anastomosis necrosis (ischemia reperfusion injury [IRI]) that developed within a month after transplantation was graded. The data were compared among the groups of veno-venous ECMO (VV-ECMO) (n = 77), veno-arterial ECMO (VA-ECMO) (n = 14), and mechanical ventilation (MV, n = 33).
Results
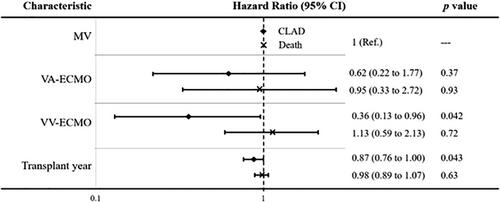
Higher levels of support (VV/VA-ECMO) were associated with a lower incidence of PGD3, which was highest in recipients on MV only (M2 = 19.54, r = −0.41, p < 0.001). In a multivariable competing risk analysis, VV-ECMO was protective against chronic allograft dysfunction (CLAD) relative to the MV group (HR: 0.36 [0.13–0.96], p = 0.042). There was no relationship between posttransplant support and survival.
Conclusion
This study suggests posttransplant VV-ECMO support in patients who develop PGD3 may confer a protective advantage over MV alone in the prevention of ischemic reperfusion injury. VV-ECMO was associated with lower IRI grades and lower rates of BOS after transplantation. Future studies investigating the causal mechanisms are warranted.
期刊介绍:
Clinical Transplantation: The Journal of Clinical and Translational Research aims to serve as a channel of rapid communication for all those involved in the care of patients who require, or have had, organ or tissue transplants, including: kidney, intestine, liver, pancreas, islets, heart, heart valves, lung, bone marrow, cornea, skin, bone, and cartilage, viable or stored.
Published monthly, Clinical Transplantation’s scope is focused on the complete spectrum of present transplant therapies, as well as also those that are experimental or may become possible in future. Topics include:
Immunology and immunosuppression;
Patient preparation;
Social, ethical, and psychological issues;
Complications, short- and long-term results;
Artificial organs;
Donation and preservation of organ and tissue;
Translational studies;
Advances in tissue typing;
Updates on transplant pathology;.
Clinical and translational studies are particularly welcome, as well as focused reviews. Full-length papers and short communications are invited. Clinical reviews are encouraged, as well as seminal papers in basic science which might lead to immediate clinical application. Prominence is regularly given to the results of cooperative surveys conducted by the organ and tissue transplant registries.
Clinical Transplantation: The Journal of Clinical and Translational Research is essential reading for clinicians and researchers in the diverse field of transplantation: surgeons; clinical immunologists; cryobiologists; hematologists; gastroenterologists; hepatologists; pulmonologists; nephrologists; cardiologists; and endocrinologists. It will also be of interest to sociologists, psychologists, research workers, and to all health professionals whose combined efforts will improve the prognosis of transplant recipients.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
