Impact of access to coronary angiography and percutaneous coronary intervention on in-hospital and five-year mortality in patients with acute coronary syndrome: a propensity-matched cohort study in Thailand.
Ponlagrit Kumwichar, Jutatip Thungthong, Tippawan Liabsuetrakul, Hisateru Tachimori, Mariko Hosozawa, Eiko Saito, Yuta Taniguchi, Virasakdi Chongsuvivatwong, Hiroyasu Iso
{"title":"Impact of access to coronary angiography and percutaneous coronary intervention on in-hospital and five-year mortality in patients with acute coronary syndrome: a propensity-matched cohort study in Thailand.","authors":"Ponlagrit Kumwichar, Jutatip Thungthong, Tippawan Liabsuetrakul, Hisateru Tachimori, Mariko Hosozawa, Eiko Saito, Yuta Taniguchi, Virasakdi Chongsuvivatwong, Hiroyasu Iso","doi":"10.1186/s41256-024-00390-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Coronary artery angiography (CAG) and percutaneous coronary intervention (PCI) are superior to non-invasive approaches in reducing mortality in patients with ST-segment elevation myocardial infarction (STEMI). However, their efficacy remains uncertain in non-ST-elevation acute coronary syndromes (NSTE-ACS) and limited in low-resource settings. This study aimed to compare in-hospital and 5-year mortality rates between patients with a first event of STEMI and NSTE-ACS who underwent CAG and PCI and those with similar severity who did not undergo CAG and PCI.</p><p><strong>Methods: </strong>A propensity-matched retrospective cohort study was conducted using population-based claims data of national universal coverage of Thailand for identification of patients with acute coronary syndromes. The mortality of recruited patients was additionally linked to the national database of vital registration. Patients aged ≥ 40 years who were hospitalized for STEMI and NSTE-ACS in 2017, with a focus on access to CAG and PCI were included. For each condition either STEMI or NSTE-ACS, patients who underwent CAG and PCI were matched to those who did not undergo using propensity score matching (PSM) to balance measured confounders, such as age, sex, and underlying conditions. In-hospital mortality rate ratio and 5-year mortality were analyzed as measures.</p><p><strong>Results: </strong>Through PSM, 2,702 non-intervention STEMI patients were paired with an equal number of intervention patients, and similarly, 5,072 non-intervention NSTE-ACS patients were matched with an equivalent group who received interventions. For patients with STEMI, the in-hospital mortality rate ratio (95% confidence interval (CI)) for those who underwent CAG and PCI compared to those who did not was 30.1% (30.0%, 30.2%). Similar trends were observed in patients with NSTE-ACS with a mortality rate of 34.7% (34.6%, 34.8%). For the five-year mortality comparison, the hazard ratios (95% CI) of mortality after discharge were 0.55 (0.50, 0.62) for STEMI and 0.57 (0.54, 0.61) for NSTE-ACS cases.</p><p><strong>Conclusions: </strong>Access to CAG and PCI was significantly associated with lower in-hospital and 5-year mortality rates in patients who experienced their first event of ACS, despite the limited availability of some unmeasured or residual confounders. Healthcare systems should expand their resources for CAG and PCI in Thailand and other countries to equitably enhance longevity.</p>","PeriodicalId":52405,"journal":{"name":"Global Health Research and Policy","volume":"9 1","pages":"48"},"PeriodicalIF":4.6000,"publicationDate":"2024-11-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11575078/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Health Research and Policy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s41256-024-00390-x","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Coronary artery angiography (CAG) and percutaneous coronary intervention (PCI) are superior to non-invasive approaches in reducing mortality in patients with ST-segment elevation myocardial infarction (STEMI). However, their efficacy remains uncertain in non-ST-elevation acute coronary syndromes (NSTE-ACS) and limited in low-resource settings. This study aimed to compare in-hospital and 5-year mortality rates between patients with a first event of STEMI and NSTE-ACS who underwent CAG and PCI and those with similar severity who did not undergo CAG and PCI.
Methods: A propensity-matched retrospective cohort study was conducted using population-based claims data of national universal coverage of Thailand for identification of patients with acute coronary syndromes. The mortality of recruited patients was additionally linked to the national database of vital registration. Patients aged ≥ 40 years who were hospitalized for STEMI and NSTE-ACS in 2017, with a focus on access to CAG and PCI were included. For each condition either STEMI or NSTE-ACS, patients who underwent CAG and PCI were matched to those who did not undergo using propensity score matching (PSM) to balance measured confounders, such as age, sex, and underlying conditions. In-hospital mortality rate ratio and 5-year mortality were analyzed as measures.
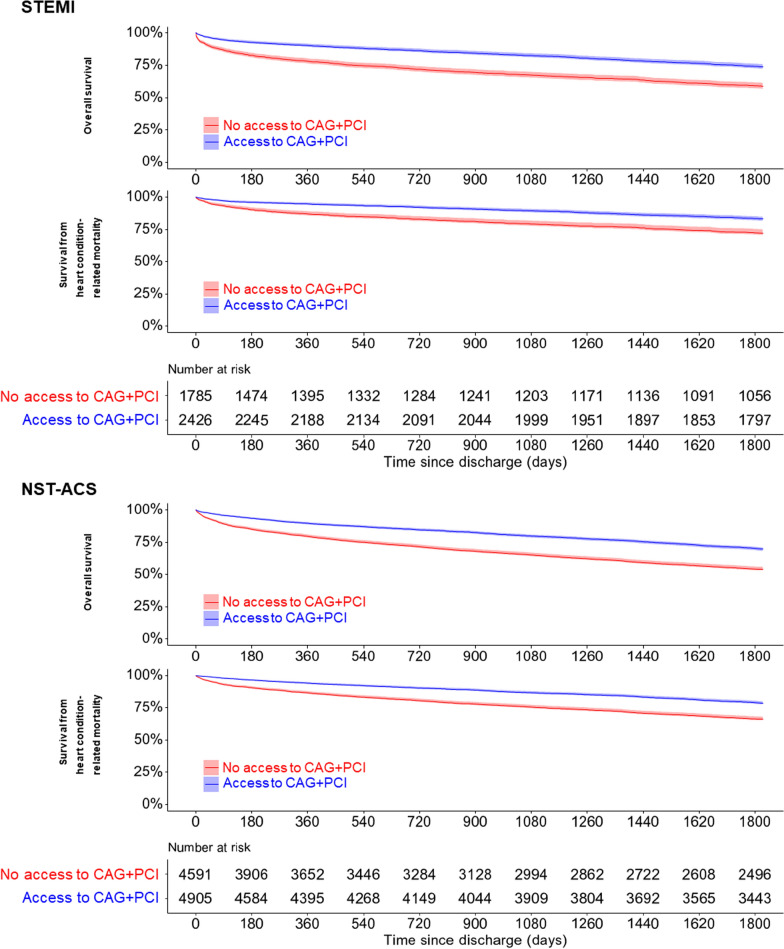
Results: Through PSM, 2,702 non-intervention STEMI patients were paired with an equal number of intervention patients, and similarly, 5,072 non-intervention NSTE-ACS patients were matched with an equivalent group who received interventions. For patients with STEMI, the in-hospital mortality rate ratio (95% confidence interval (CI)) for those who underwent CAG and PCI compared to those who did not was 30.1% (30.0%, 30.2%). Similar trends were observed in patients with NSTE-ACS with a mortality rate of 34.7% (34.6%, 34.8%). For the five-year mortality comparison, the hazard ratios (95% CI) of mortality after discharge were 0.55 (0.50, 0.62) for STEMI and 0.57 (0.54, 0.61) for NSTE-ACS cases.
Conclusions: Access to CAG and PCI was significantly associated with lower in-hospital and 5-year mortality rates in patients who experienced their first event of ACS, despite the limited availability of some unmeasured or residual confounders. Healthcare systems should expand their resources for CAG and PCI in Thailand and other countries to equitably enhance longevity.
期刊介绍:
Global Health Research and Policy, an open-access, multidisciplinary journal, publishes research on various aspects of global health, addressing topics like health equity, health systems and policy, social determinants of health, disease burden, population health, and other urgent global health issues. It serves as a forum for high-quality research focused on regional and global health improvement, emphasizing solutions for health equity.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
