Collin R Miller, Catherine Haut, Arezoo Zomorrodi, Karina Chara, Janice Wilson
{"title":"Implementation of a Neonatal Hyperbilirubinemia Clinical Pathway in a Pediatric Emergency Department.","authors":"Collin R Miller, Catherine Haut, Arezoo Zomorrodi, Karina Chara, Janice Wilson","doi":"10.1097/pq9.0000000000000774","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>High volumes and competing priorities delay care initiation for neonatal hyperbilirubinemia within the pediatric emergency department (ED). Our freestanding children's hospital developed a quality improvement project to implement a nurse-initiated neonatal hyperbilirubinemia clinical pathway (CP) intended to decrease treatment initiation and intravenous fluid (IVF) rates.</p><p><strong>Methods: </strong>A multidisciplinary team used the model for improvement to delineate and address key drivers of treatment delays. The team established a nurse-driven CP and enhanced the electronic health record to support and enforce new workflows, which included capillary specimen collection and phototherapy initiation before the first provider assessment. IVF criteria and laboratory evaluation were standardized. The primary aim was to decrease the time to initiation of phototherapy from a mean of 136 to 60 minutes after ED arrival for 6 months. The secondary aim was to decrease the proportion of patients obtaining IVF from 31% to 15% for the same time frame.</p><p><strong>Results: </strong>ED arrival to phototherapy initiation decreased from 136 to 49 minutes. The IVF rate decreased from 31% to 12%. ED length of stay decreased from 185 to 122 minutes. Hospital length of stay remained unchanged.</p><p><strong>Conclusions: </strong>A nurse-initiated CP for neonates with hyperbilirubinemia improved time-to-care initiation and ED throughput while decreasing unnecessary IVF administration.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 6","pages":"e774"},"PeriodicalIF":1.1000,"publicationDate":"2024-11-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11578199/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000774","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: High volumes and competing priorities delay care initiation for neonatal hyperbilirubinemia within the pediatric emergency department (ED). Our freestanding children's hospital developed a quality improvement project to implement a nurse-initiated neonatal hyperbilirubinemia clinical pathway (CP) intended to decrease treatment initiation and intravenous fluid (IVF) rates.
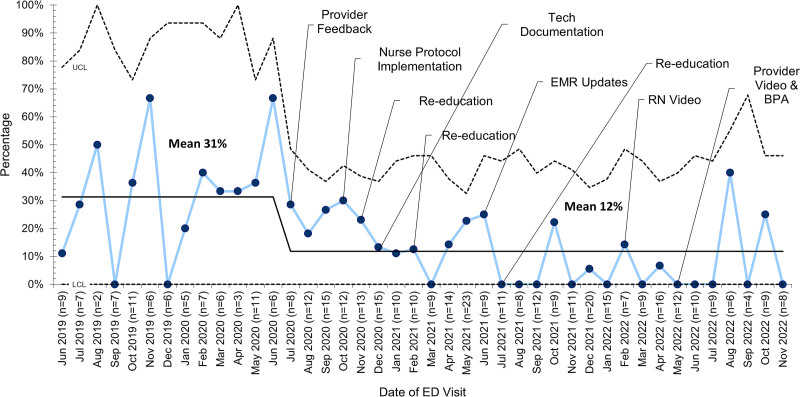
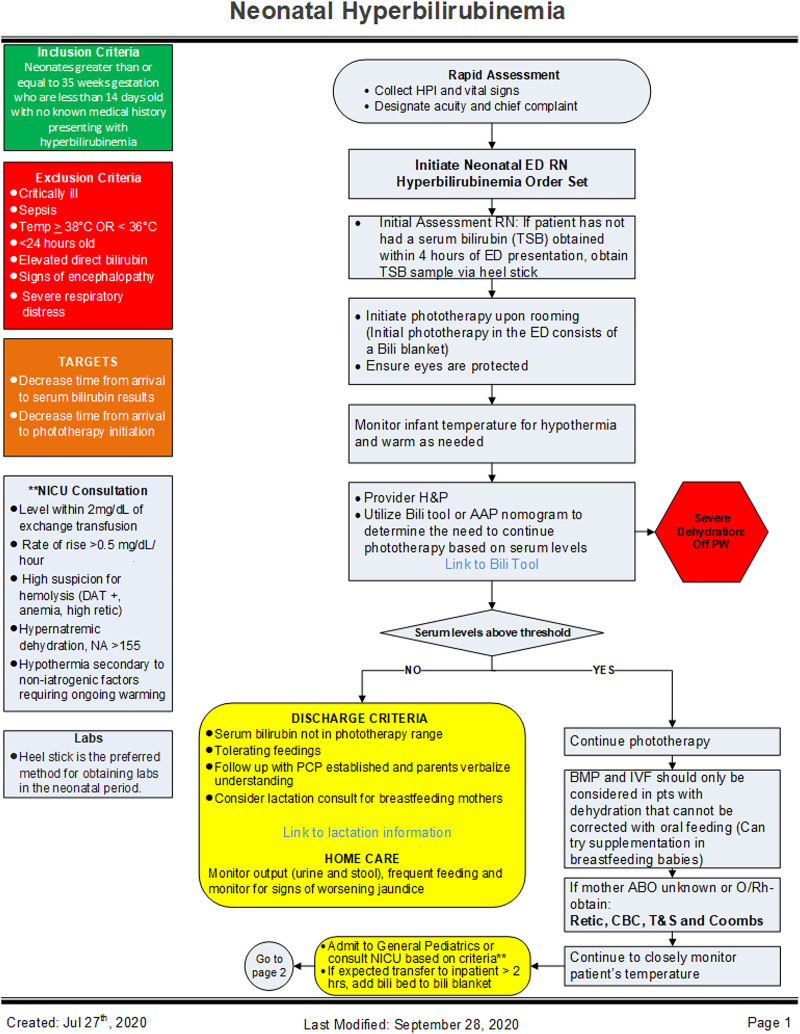
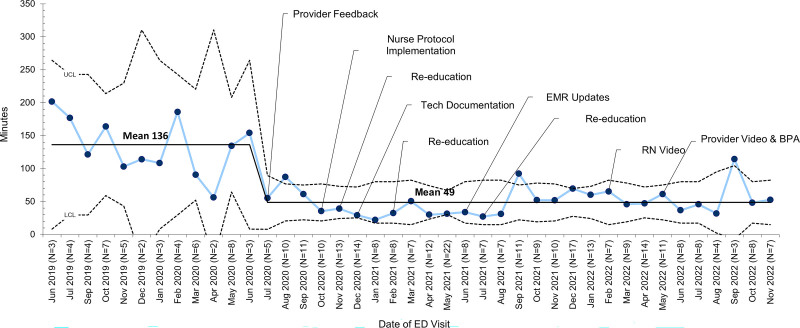
Methods: A multidisciplinary team used the model for improvement to delineate and address key drivers of treatment delays. The team established a nurse-driven CP and enhanced the electronic health record to support and enforce new workflows, which included capillary specimen collection and phototherapy initiation before the first provider assessment. IVF criteria and laboratory evaluation were standardized. The primary aim was to decrease the time to initiation of phototherapy from a mean of 136 to 60 minutes after ED arrival for 6 months. The secondary aim was to decrease the proportion of patients obtaining IVF from 31% to 15% for the same time frame.
Results: ED arrival to phototherapy initiation decreased from 136 to 49 minutes. The IVF rate decreased from 31% to 12%. ED length of stay decreased from 185 to 122 minutes. Hospital length of stay remained unchanged.
Conclusions: A nurse-initiated CP for neonates with hyperbilirubinemia improved time-to-care initiation and ED throughput while decreasing unnecessary IVF administration.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
