Using Quality Improvement to Design and Evaluate an Outpatient Day Treatment Pathway for Pediatric Patients with Diabetes Mellitus Requiring Insulin Initiation.
Svetlana Azova, Charumathi Baskaran, Sara Einis, Jennifer Fortin, Marisa Silva, Miriam Gorman, Benjamin Ethier, Sonal Nanavati, Olivia Sterns, Katharine Garvey, Erinn T Rhodes
{"title":"Using Quality Improvement to Design and Evaluate an Outpatient Day Treatment Pathway for Pediatric Patients with Diabetes Mellitus Requiring Insulin Initiation.","authors":"Svetlana Azova, Charumathi Baskaran, Sara Einis, Jennifer Fortin, Marisa Silva, Miriam Gorman, Benjamin Ethier, Sonal Nanavati, Olivia Sterns, Katharine Garvey, Erinn T Rhodes","doi":"10.1097/pq9.0000000000000776","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Education and management of children with new-onset or established diabetes mellitus (DM) requiring insulin initiation do not always require hospitalization. We developed a pathway for outpatient day treatment of select patients after initial evaluation in the emergency department (ED) at a pediatric, tertiary care academic medical center.</p><p><strong>Methods: </strong>A multidisciplinary team identified key initial eligibility criteria for outpatient day treatment for insulin initiation, including absence of diabetic ketoacidosis, age ≥3 years, and plasma beta-hydroxybutyrate (BOHB) <1 mmol/L. Electronic medical record reviews and surveys administered to endocrine providers determined exclusions or reasons for nonparticipation. Refinement of the pathway occurred through iterative plan-do-study-act cycles. Statistical process control evaluated the uptake among eligible patients.</p><p><strong>Results: </strong>We launched the pathway in September 2020. Of 534 patients presenting to the ED with new-onset or established DM requiring insulin initiation in the first 2.5 years, 198 were potentially eligible for day treatment. Of these, 65 children (33%) completed the pathway. One additional patient was hospitalized following Day 1 of education due to newly identified psychosocial stressors. The increase of BOHB cutoff to 1.5 mmol/L and the option of rapid-acting insulin bolus for borderline BOHB resulted in a significant shift in utilization from a mean of 24.4% to 41.1%. Persistent barriers to participation include limited appointment availability, weekend presentation, and patient/family concerns.</p><p><strong>Conclusions: </strong>Outpatient day treatment was successful for select pediatric patients with new-onset or established DM requiring insulin initiation. However, this approach necessitates flexible resources and supportive patient messaging.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 6","pages":"e776"},"PeriodicalIF":1.1000,"publicationDate":"2024-11-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11578214/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000776","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Education and management of children with new-onset or established diabetes mellitus (DM) requiring insulin initiation do not always require hospitalization. We developed a pathway for outpatient day treatment of select patients after initial evaluation in the emergency department (ED) at a pediatric, tertiary care academic medical center.
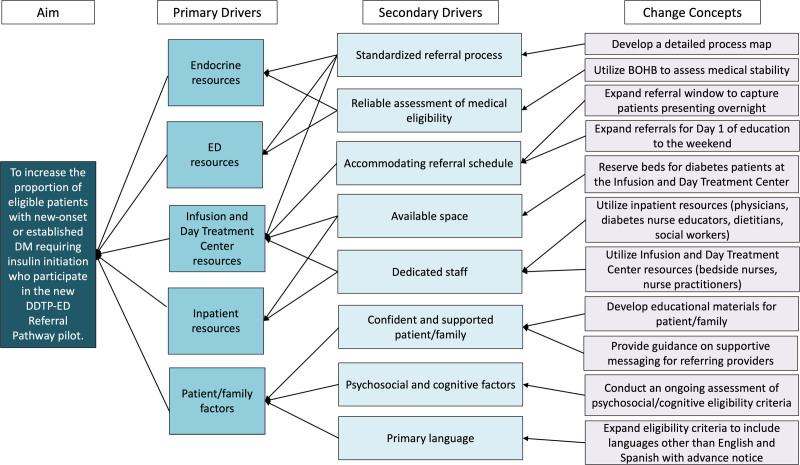
Methods: A multidisciplinary team identified key initial eligibility criteria for outpatient day treatment for insulin initiation, including absence of diabetic ketoacidosis, age ≥3 years, and plasma beta-hydroxybutyrate (BOHB) <1 mmol/L. Electronic medical record reviews and surveys administered to endocrine providers determined exclusions or reasons for nonparticipation. Refinement of the pathway occurred through iterative plan-do-study-act cycles. Statistical process control evaluated the uptake among eligible patients.
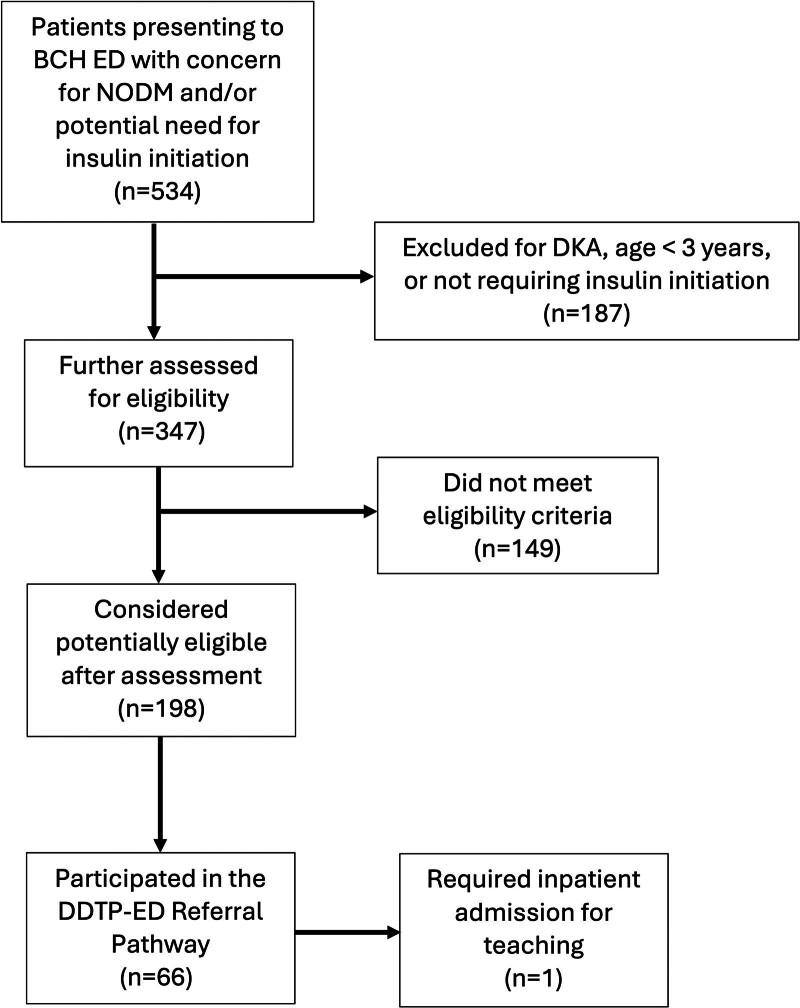
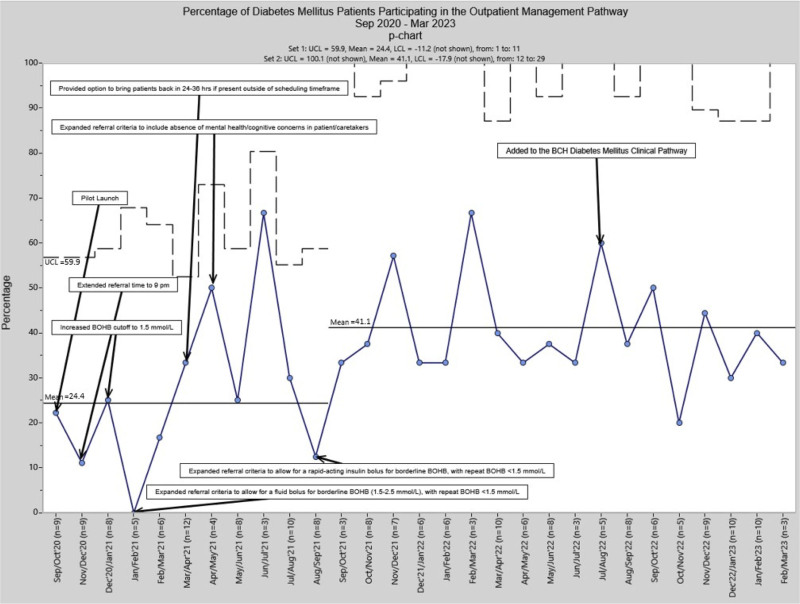
Results: We launched the pathway in September 2020. Of 534 patients presenting to the ED with new-onset or established DM requiring insulin initiation in the first 2.5 years, 198 were potentially eligible for day treatment. Of these, 65 children (33%) completed the pathway. One additional patient was hospitalized following Day 1 of education due to newly identified psychosocial stressors. The increase of BOHB cutoff to 1.5 mmol/L and the option of rapid-acting insulin bolus for borderline BOHB resulted in a significant shift in utilization from a mean of 24.4% to 41.1%. Persistent barriers to participation include limited appointment availability, weekend presentation, and patient/family concerns.
Conclusions: Outpatient day treatment was successful for select pediatric patients with new-onset or established DM requiring insulin initiation. However, this approach necessitates flexible resources and supportive patient messaging.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
