Marco Finati, Alex Stephens, Giuseppe Ottone Cirulli, Giuseppe Chiarelli, Shane Tinsley, Chase Morrison, Akshay Sood, Nicolò Buffi, Giovanni Lughezzani, Andrea Salonia, Alberto Briganti, Francesco Montorsi, Gian Maria Busetto, Craig Rogers, Giuseppe Carrieri, Firas Abdollah
{"title":"Association of race and area of deprivation index with prostate cancer incidence and lethality: results from a contemporary North American cohort.","authors":"Marco Finati, Alex Stephens, Giuseppe Ottone Cirulli, Giuseppe Chiarelli, Shane Tinsley, Chase Morrison, Akshay Sood, Nicolò Buffi, Giovanni Lughezzani, Andrea Salonia, Alberto Briganti, Francesco Montorsi, Gian Maria Busetto, Craig Rogers, Giuseppe Carrieri, Firas Abdollah","doi":"10.1093/jncics/pkae112","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Socioeconomic and demographic factors contribute to disparity in prostate cancer (PCa) outcomes. We examined the impact of Area of Deprivation Index (ADI) and race on PCa incidence and lethality in a North American cohort.</p><p><strong>Methods: </strong>Our cohort included men who received at least 1 prostate-Specifig Antigen (pSA) test within our Health System (1995-2022). An ADI score was assigned to each patient based on their residential census block, ranked as a percentile of deprivation relative to the national level. Individuals were further categorized into quartiles, where the fourth one (ADI 75-100) represented those living in the most deprived areas. We investigated PCa incidence and lethality, using cumulative incidence estimates and competing-risk regression. An ADI × Race interaction term examined whether the relationship between ADI and outcomes varied based on race.</p><p><strong>Results: </strong>We included 134 366 patients, 25% of whom were non-Hispanic Black (NHB). Median (IQR) follow-up was 8.8 (5-17) years. At multivariate analysis, individuals from the third quartile (ADI 50-74, 95% CI = 0.83 to 0.95) and the fourth quartile (ADI ≥75, 95% CI = 0.75 to 0.86) showed significant reduced hazard ratios for PCa incidence, when compared with the first quartile (ADI <25, all P < .001). In contrast to the overall cohort, PCa incidence increased with ADI in NHB men, who were persistently at higher hazard for both PCa incidence and lethality than non-Hispanic White (NHW), across all ADI strata (all P < .001).</p><p><strong>Conclusions: </strong>Living in more deprived areas was associated with lower PCa incidence and higher lethal disease rate. Conversely, PCa incidence increased with ADI for NHB, who consistently showed worse outcomes than NHW individuals, regardless of ADI.</p>","PeriodicalId":14681,"journal":{"name":"JNCI Cancer Spectrum","volume":" ","pages":""},"PeriodicalIF":4.1000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11658688/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JNCI Cancer Spectrum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jncics/pkae112","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Socioeconomic and demographic factors contribute to disparity in prostate cancer (PCa) outcomes. We examined the impact of Area of Deprivation Index (ADI) and race on PCa incidence and lethality in a North American cohort.
Methods: Our cohort included men who received at least 1 prostate-Specifig Antigen (pSA) test within our Health System (1995-2022). An ADI score was assigned to each patient based on their residential census block, ranked as a percentile of deprivation relative to the national level. Individuals were further categorized into quartiles, where the fourth one (ADI 75-100) represented those living in the most deprived areas. We investigated PCa incidence and lethality, using cumulative incidence estimates and competing-risk regression. An ADI × Race interaction term examined whether the relationship between ADI and outcomes varied based on race.
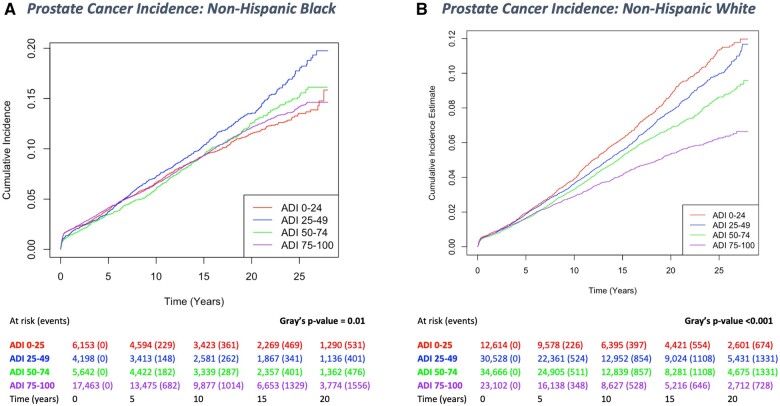
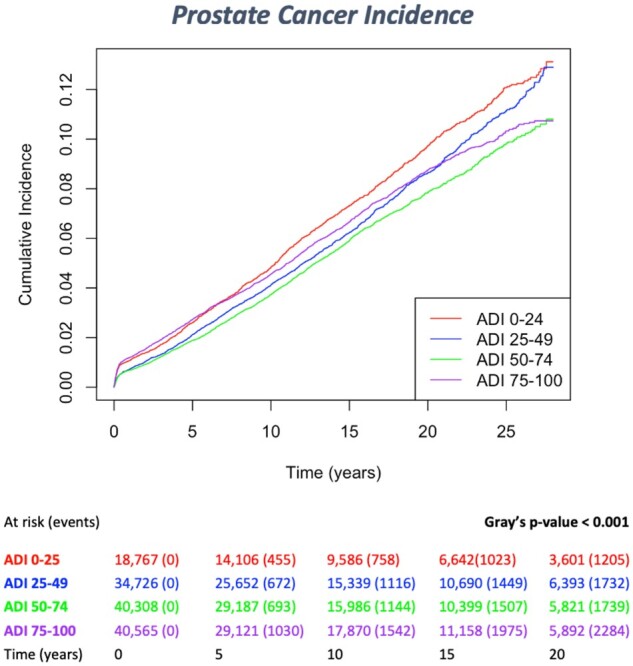
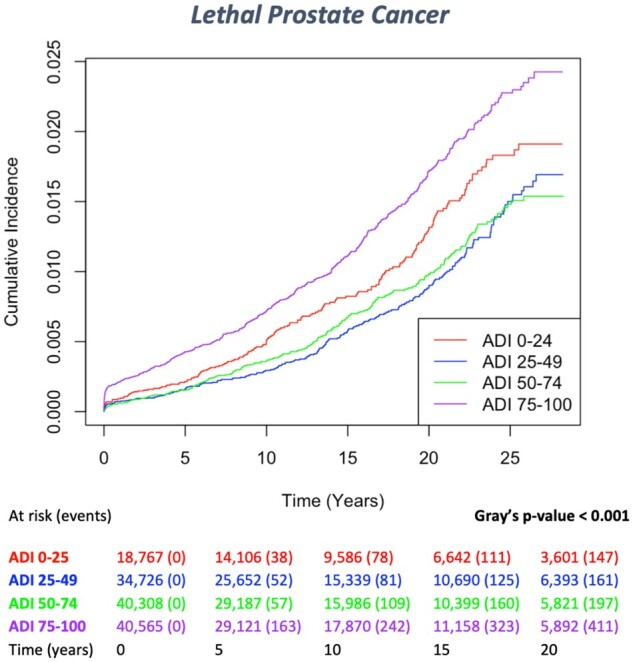
Results: We included 134 366 patients, 25% of whom were non-Hispanic Black (NHB). Median (IQR) follow-up was 8.8 (5-17) years. At multivariate analysis, individuals from the third quartile (ADI 50-74, 95% CI = 0.83 to 0.95) and the fourth quartile (ADI ≥75, 95% CI = 0.75 to 0.86) showed significant reduced hazard ratios for PCa incidence, when compared with the first quartile (ADI <25, all P < .001). In contrast to the overall cohort, PCa incidence increased with ADI in NHB men, who were persistently at higher hazard for both PCa incidence and lethality than non-Hispanic White (NHW), across all ADI strata (all P < .001).
Conclusions: Living in more deprived areas was associated with lower PCa incidence and higher lethal disease rate. Conversely, PCa incidence increased with ADI for NHB, who consistently showed worse outcomes than NHW individuals, regardless of ADI.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
