Vera Vik Bjarkø, Eirin Beate Haug, Arnulf Langhammer, Paz Lopez-Doriga Ruiz, Sofia Carlsson, Kare I Birkeland, Tore Julsrud Berg, Elin Pettersen Sørgjerd, Valeriya Lyssenko, Bjørn Olav Åsvold
{"title":"Clinical utility of novel diabetes subgroups in predicting vascular complications and mortality: up to 25 years of follow-up of the HUNT Study.","authors":"Vera Vik Bjarkø, Eirin Beate Haug, Arnulf Langhammer, Paz Lopez-Doriga Ruiz, Sofia Carlsson, Kare I Birkeland, Tore Julsrud Berg, Elin Pettersen Sørgjerd, Valeriya Lyssenko, Bjørn Olav Åsvold","doi":"10.1136/bmjdrc-2024-004493","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Cluster analysis has previously revealed five reproducible subgroups of diabetes, differing in risks of diabetic complications. We aimed to examine the clusters' predictive ability for vascular complications as compared with established risk factors in a general adult diabetes population.</p><p><strong>Research design and methods: </strong>Participants from the second (HUNT2, 1995-1997) and third (HUNT3, 2006-2008) surveys of the Norwegian population-based Trøndelag Health Study (HUNT Study) with adult-onset diabetes were included (n=1899). To identify diabetes subgroups, we used the same variables (age at diagnosis, body mass index, HbA1c, homeostasis model assessment estimates of beta cell function and insulin resistance, and glutamic acid decarboxylase antibodies) and the same data-driven clustering technique as in previous studies. We used Cox proportional hazards models to investigate associations between clusters and risks of vascular complications and mortality. We estimated the C-index and R<sup>2</sup> to compare predictive abilities of the clusters to those of established risk factors as continuous variables. All models included adjustment for age, sex, diabetes duration and time of inclusion.</p><p><strong>Results: </strong>We reproduced five subgroups with similar key characteristics as identified in previous studies. During median follow-up of 9-13 years (differing between outcomes), the clusters were associated with different risks of vascular complications and all-cause mortality. However, in prediction models, individual established risk factors were at least as good predictors as cluster assignment for all outcomes. For example, for retinopathy, the C-index for the model including clusters (0.65 (95% CI 0.63 to 0.68)) was similar to that of HbA1c (0.65 (95% CI 0.63 to 0.68)) or fasting C-peptide (0.66 (95% CI 0.63 to 0.68)) alone. For chronic kidney disease, the C-index for clusters (0.74 (95% CI 0.72 to 0.76)) was similar to that of triglyceride/high-density lipoprotein ratio (0.74 (95% CI 0.71 to 0.76)) or fasting C-peptide (0.74 (95% CI 0.72 to 0.76)), and baseline estimated glomerular filtration rate yielded a C-index of 0.76 (95% CI 0.74 to 0.78).</p><p><strong>Conclusions: </strong>Cluster assignment did not provide better prediction of vascular complications or all-cause mortality compared with established risk factors.</p>","PeriodicalId":9151,"journal":{"name":"BMJ Open Diabetes Research & Care","volume":"12 6","pages":""},"PeriodicalIF":4.1000,"publicationDate":"2024-11-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11590787/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Diabetes Research & Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjdrc-2024-004493","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Cluster analysis has previously revealed five reproducible subgroups of diabetes, differing in risks of diabetic complications. We aimed to examine the clusters' predictive ability for vascular complications as compared with established risk factors in a general adult diabetes population.
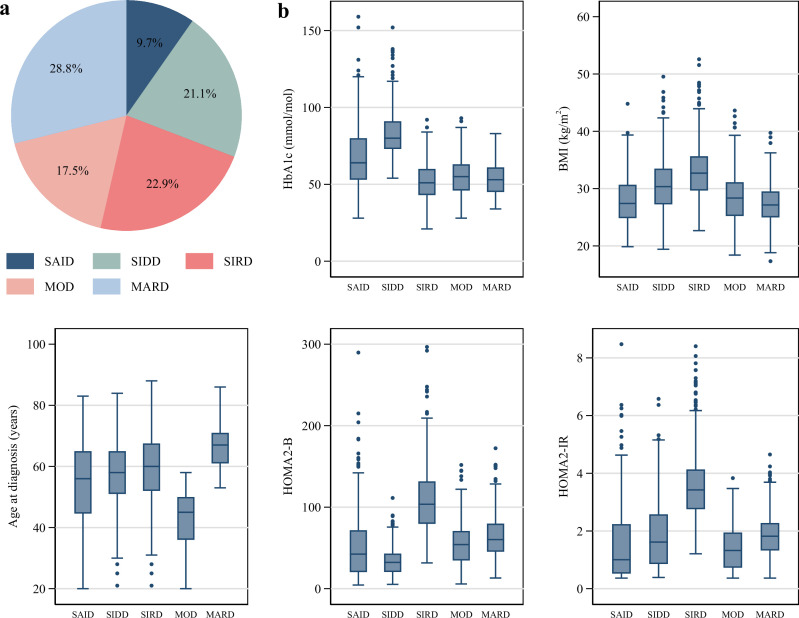
Research design and methods: Participants from the second (HUNT2, 1995-1997) and third (HUNT3, 2006-2008) surveys of the Norwegian population-based Trøndelag Health Study (HUNT Study) with adult-onset diabetes were included (n=1899). To identify diabetes subgroups, we used the same variables (age at diagnosis, body mass index, HbA1c, homeostasis model assessment estimates of beta cell function and insulin resistance, and glutamic acid decarboxylase antibodies) and the same data-driven clustering technique as in previous studies. We used Cox proportional hazards models to investigate associations between clusters and risks of vascular complications and mortality. We estimated the C-index and R2 to compare predictive abilities of the clusters to those of established risk factors as continuous variables. All models included adjustment for age, sex, diabetes duration and time of inclusion.
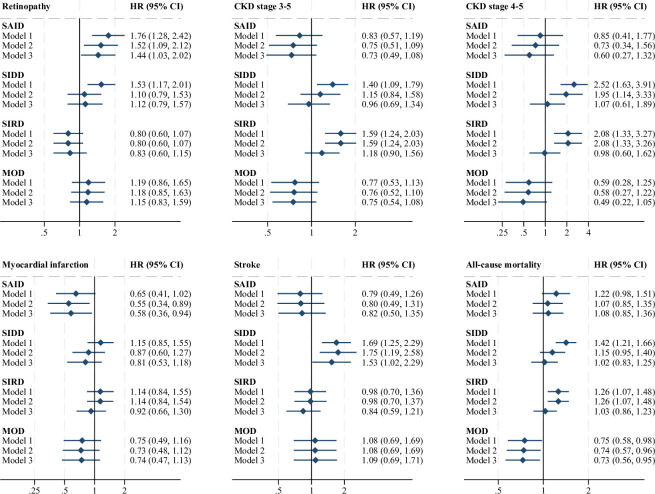
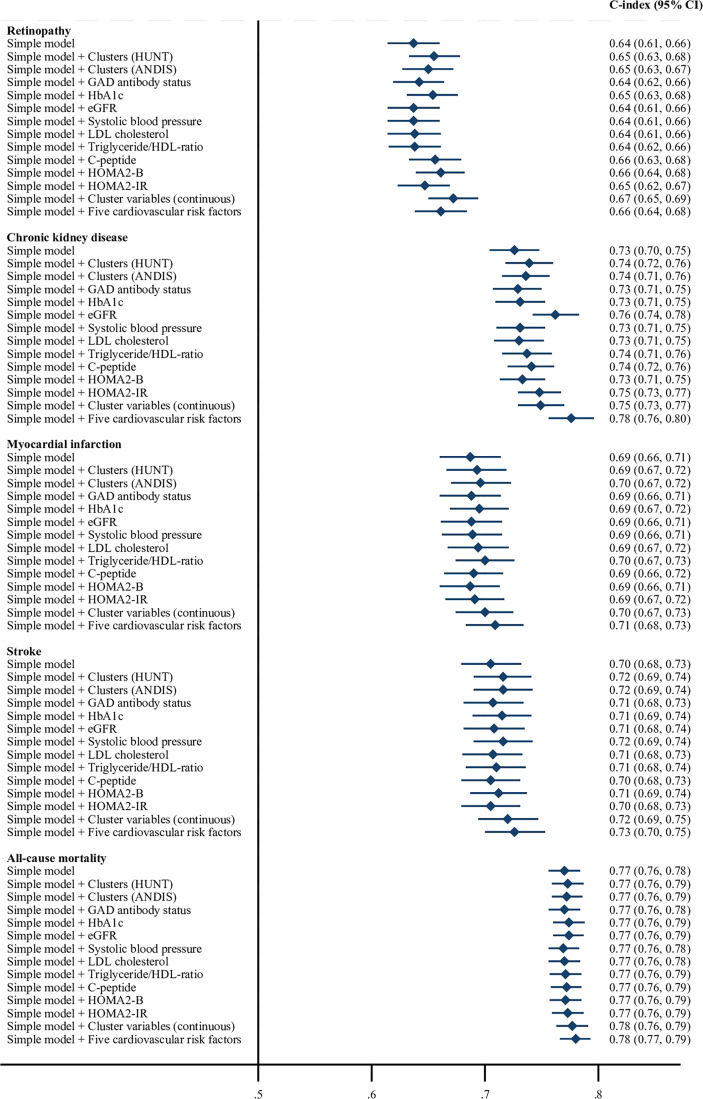
Results: We reproduced five subgroups with similar key characteristics as identified in previous studies. During median follow-up of 9-13 years (differing between outcomes), the clusters were associated with different risks of vascular complications and all-cause mortality. However, in prediction models, individual established risk factors were at least as good predictors as cluster assignment for all outcomes. For example, for retinopathy, the C-index for the model including clusters (0.65 (95% CI 0.63 to 0.68)) was similar to that of HbA1c (0.65 (95% CI 0.63 to 0.68)) or fasting C-peptide (0.66 (95% CI 0.63 to 0.68)) alone. For chronic kidney disease, the C-index for clusters (0.74 (95% CI 0.72 to 0.76)) was similar to that of triglyceride/high-density lipoprotein ratio (0.74 (95% CI 0.71 to 0.76)) or fasting C-peptide (0.74 (95% CI 0.72 to 0.76)), and baseline estimated glomerular filtration rate yielded a C-index of 0.76 (95% CI 0.74 to 0.78).
Conclusions: Cluster assignment did not provide better prediction of vascular complications or all-cause mortality compared with established risk factors.
简介聚类分析曾揭示了五个可重复的糖尿病亚组,它们在糖尿病并发症风险方面存在差异。我们的目的是在普通成人糖尿病人群中,与已确定的风险因素相比,研究这些分组对血管并发症的预测能力:研究对象包括挪威特伦德拉格健康研究(HUNT研究)第二次(HUNT2,1995-1997年)和第三次(HUNT3,2006-2008年)调查中的成年糖尿病患者(1899人)。为了确定糖尿病亚组,我们使用了与以往研究相同的变量(诊断年龄、体重指数、HbA1c、β细胞功能和胰岛素抵抗的稳态模型评估估计值以及谷氨酸脱羧酶抗体)和数据驱动的聚类技术。我们使用 Cox 比例危险模型来研究聚类与血管并发症和死亡风险之间的关联。我们估算了 C 指数和 R2,以比较聚类与作为连续变量的既定风险因素的预测能力。所有模型都对年龄、性别、糖尿病病程和纳入时间进行了调整:我们再现了五个亚组,其主要特征与之前研究中确定的相似。在中位随访 9-13 年期间(不同结果之间存在差异),这些分组与不同的血管并发症和全因死亡率风险相关。然而,在预测模型中,单个既定风险因素对所有结果的预测效果至少与分组分配一样好。例如,就视网膜病变而言,包括分组在内的模型的 C 指数(0.65(95% CI 0.63 至 0.68))与单独的 HbA1c(0.65(95% CI 0.63 至 0.68))或空腹 C 肽(0.66(95% CI 0.63 至 0.68))相似。对于慢性肾脏病,分组的C指数(0.74(95% CI 0.72至0.76))与甘油三酯/高密度脂蛋白比值(0.74(95% CI 0.71至0.76))或空腹C肽(0.74(95% CI 0.72至0.76))相似,基线肾小球滤过率估计值的C指数为0.76(95% CI 0.74至0.78):结论:与既定的风险因素相比,分组分配并不能更好地预测血管并发症或全因死亡率。
期刊介绍:
BMJ Open Diabetes Research & Care is an open access journal committed to publishing high-quality, basic and clinical research articles regarding type 1 and type 2 diabetes, and associated complications. Only original content will be accepted, and submissions are subject to rigorous peer review to ensure the publication of
high-quality — and evidence-based — original research articles.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
