Cost-effectiveness of viral load testing for transitioning antiretroviral therapy-experienced children to dolutegravir in South Africa: a modelling analysis.
Isaac Ravi Brenner, Clare F Flanagan, Martina Penazzato, Karen A Webb, Stephanie B Horsfall, Emily P Hyle, Elaine Abrams, Jason Bacha, Anne M Neilan, Intira Jeannie Collins, Sophie Desmonde, Siobhan Crichton, Mary-Ann Davies, Kenneth A Freedberg, Andrea L Ciaranello
{"title":"Cost-effectiveness of viral load testing for transitioning antiretroviral therapy-experienced children to dolutegravir in South Africa: a modelling analysis.","authors":"Isaac Ravi Brenner, Clare F Flanagan, Martina Penazzato, Karen A Webb, Stephanie B Horsfall, Emily P Hyle, Elaine Abrams, Jason Bacha, Anne M Neilan, Intira Jeannie Collins, Sophie Desmonde, Siobhan Crichton, Mary-Ann Davies, Kenneth A Freedberg, Andrea L Ciaranello","doi":"10.1016/S2214-109X(24)00381-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>For children with HIV on antiretroviral therapy (ART), transitioning to dolutegravir-containing regimens is recommended. The aim of this study was to assess whether introducing viral load testing to inform new nucleoside or nucleotide reverse transcriptase inhibitors (NRTIs) for children with HIV and viraemia alongside dolutegravir-based ART is beneficial and of good economic value.</p><p><strong>Methods: </strong>We used the Cost-Effectiveness of Preventing AIDS Complications-Pediatric model to project clinical and cost implications of three strategies among a simulated cohort of South African children aged 8 years with HIV receiving abacavir-lamivudine-efavirenz: (1) continue current ART (no dolutegravir; abacavir-lamivudine-efavirenz); (2) transition all children with HIV to dolutegravir, keeping current NRTIs (dolutegravir; abacavir-lamivudine-dolutegravir); or (3) transition to dolutegravir based on viral load testing (viral load plus dolutegravir), keeping current NRTIs if virologically suppressed (abacavir-lamivudine-dolutegravir, 70% of cohort) or switching abacavir to zidovudine (zidovudine) if viraemic (zidovudine-lamivudine-dolutegravir, 30%). We assumed 50% of children who had viraemia after abacavir-lamivudine exposure had NRTI resistance; with resistance, we assumed zidovudine-lamivudine-dolutegravir was more effective than abacavir-lamivudine-dolutegravir. We designated a strategy as preferred if it was most effective and least costly or had an incremental cost-effectiveness ratio less than half the South African 2020 gross domestic product per capita.</p><p><strong>Findings: </strong>Under base-case assumptions, the viral load plus dolutegravir strategy would be the most effective (projected undiscounted life expectancy of 39·72 life-years) and least costly strategy (US$24 600 per person); the no dolutegravir strategy was the least effective (34·49 life-years) and most expensive ($26 480 per person). In sensitivity analyses, the 24-week virological suppression probability and subsequent monthly virological failure risks (ie, late failure) were most influential on cost-effectiveness. Only with a high late-failure risk for zidovudine-lamivudine-dolutegravir (ie, ≥0·3% per month in the base case or >0·5% per month if abacavir also confers low virological suppression probability in the presence of NRTI resistance [65%]) would the dolutegravir strategy become preferred above the viral load plus dolutegravir strategy.</p><p><strong>Interpretation: </strong>For programmes transitioning to dolutegravir-based regimens, our model predicted that doing so would be more effective and less costly than continuing current ART regimens, regardless of NRTI choice. Whether viral load testing for children with HIV is necessary to inform NRTI choice depends substantially on the comparative outcomes of abacavir and zidovudine after switching to dolutegravir-containing ART.</p><p><strong>Funding: </strong>The Eunice Kennedy Shriver Institute for Child Health and Human Development, the National Institute of Allergy and Infectious Diseases, the Massachusetts General Hospital Executive Committee on Research, the Massachusetts General Hospital, and the Medical Research Council.</p>","PeriodicalId":48783,"journal":{"name":"Lancet Global Health","volume":"12 12","pages":"e2068-e2079"},"PeriodicalIF":19.9000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11584319/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lancet Global Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/S2214-109X(24)00381-4","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: For children with HIV on antiretroviral therapy (ART), transitioning to dolutegravir-containing regimens is recommended. The aim of this study was to assess whether introducing viral load testing to inform new nucleoside or nucleotide reverse transcriptase inhibitors (NRTIs) for children with HIV and viraemia alongside dolutegravir-based ART is beneficial and of good economic value.
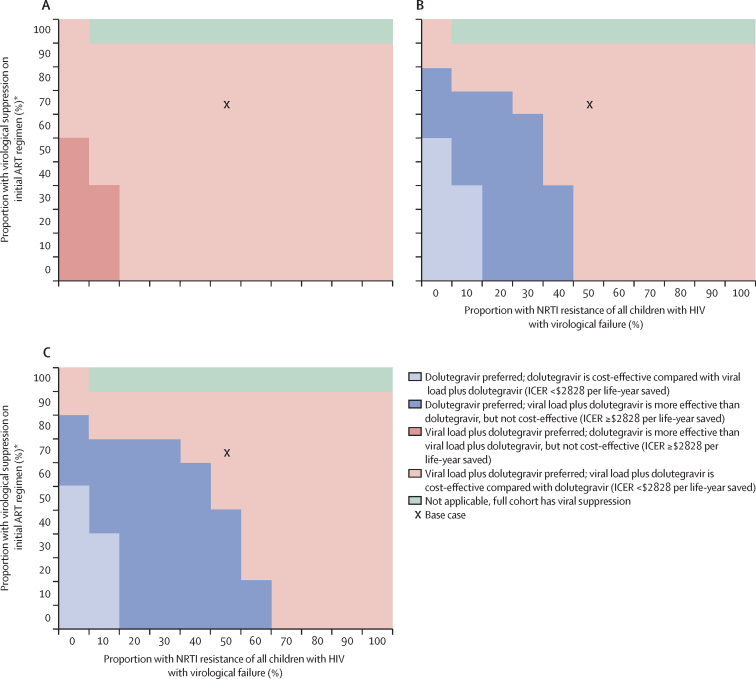
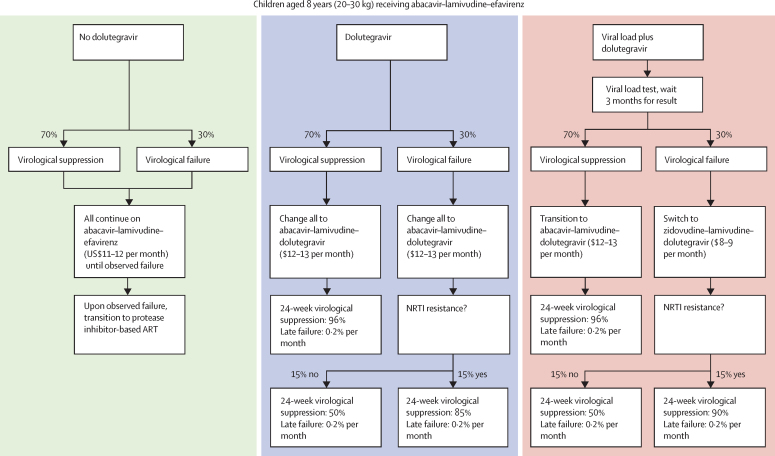
Methods: We used the Cost-Effectiveness of Preventing AIDS Complications-Pediatric model to project clinical and cost implications of three strategies among a simulated cohort of South African children aged 8 years with HIV receiving abacavir-lamivudine-efavirenz: (1) continue current ART (no dolutegravir; abacavir-lamivudine-efavirenz); (2) transition all children with HIV to dolutegravir, keeping current NRTIs (dolutegravir; abacavir-lamivudine-dolutegravir); or (3) transition to dolutegravir based on viral load testing (viral load plus dolutegravir), keeping current NRTIs if virologically suppressed (abacavir-lamivudine-dolutegravir, 70% of cohort) or switching abacavir to zidovudine (zidovudine) if viraemic (zidovudine-lamivudine-dolutegravir, 30%). We assumed 50% of children who had viraemia after abacavir-lamivudine exposure had NRTI resistance; with resistance, we assumed zidovudine-lamivudine-dolutegravir was more effective than abacavir-lamivudine-dolutegravir. We designated a strategy as preferred if it was most effective and least costly or had an incremental cost-effectiveness ratio less than half the South African 2020 gross domestic product per capita.
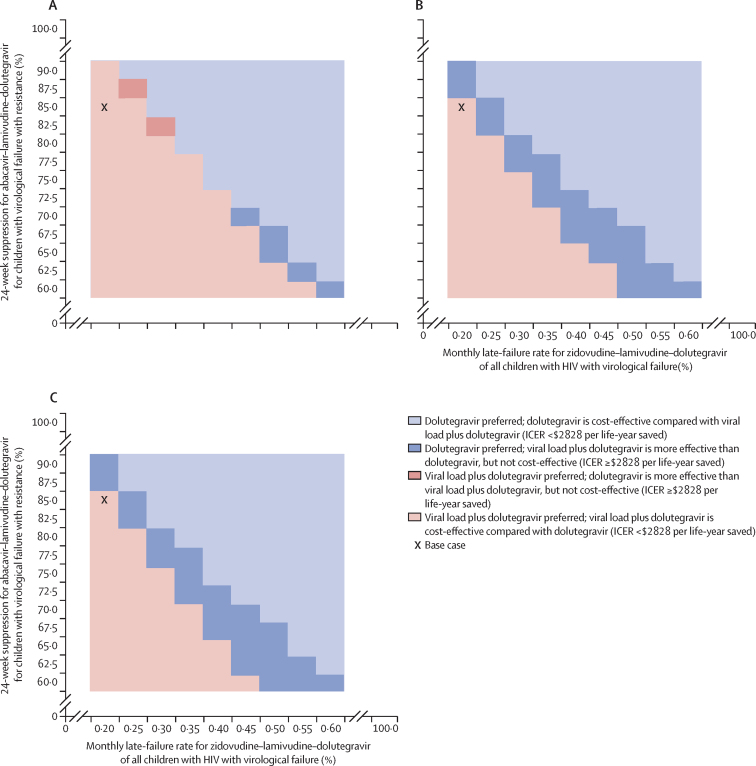
Findings: Under base-case assumptions, the viral load plus dolutegravir strategy would be the most effective (projected undiscounted life expectancy of 39·72 life-years) and least costly strategy (US$24 600 per person); the no dolutegravir strategy was the least effective (34·49 life-years) and most expensive ($26 480 per person). In sensitivity analyses, the 24-week virological suppression probability and subsequent monthly virological failure risks (ie, late failure) were most influential on cost-effectiveness. Only with a high late-failure risk for zidovudine-lamivudine-dolutegravir (ie, ≥0·3% per month in the base case or >0·5% per month if abacavir also confers low virological suppression probability in the presence of NRTI resistance [65%]) would the dolutegravir strategy become preferred above the viral load plus dolutegravir strategy.
Interpretation: For programmes transitioning to dolutegravir-based regimens, our model predicted that doing so would be more effective and less costly than continuing current ART regimens, regardless of NRTI choice. Whether viral load testing for children with HIV is necessary to inform NRTI choice depends substantially on the comparative outcomes of abacavir and zidovudine after switching to dolutegravir-containing ART.
Funding: The Eunice Kennedy Shriver Institute for Child Health and Human Development, the National Institute of Allergy and Infectious Diseases, the Massachusetts General Hospital Executive Committee on Research, the Massachusetts General Hospital, and the Medical Research Council.
期刊介绍:
The Lancet Global Health is an online publication that releases monthly open access (subscription-free) issues.Each issue includes original research, commentary, and correspondence.In addition to this, the publication also provides regular blog posts.
The main focus of The Lancet Global Health is on disadvantaged populations, which can include both entire economic regions and marginalized groups within prosperous nations.The publication prefers to cover topics related to reproductive, maternal, neonatal, child, and adolescent health; infectious diseases (including neglected tropical diseases); non-communicable diseases; mental health; the global health workforce; health systems; surgery; and health policy.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
