Julius Watrinet, Daniel Berger, Philipp Blum, Matthias P Fabritius, Jörg Arnholdt, Rolf Schipp, Wolfgang Reng, Paul Reidler
{"title":"Fractures in Oxford unicompartmental knee arthroplasty are associated with a decreased medial keel-cortex distance of the tibial implant.","authors":"Julius Watrinet, Daniel Berger, Philipp Blum, Matthias P Fabritius, Jörg Arnholdt, Rolf Schipp, Wolfgang Reng, Paul Reidler","doi":"10.1186/s43019-024-00237-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This retrospective single-center study aimed to investigate incidence and risk factors influencing tibial periprosthetic fractures (TPF) in Oxford unicompartmental knee arthroplasty (UKA), with a specific focus on tibial component positioning and sizing.</p><p><strong>Methods: </strong>A total of 2063 patients with medial UKA using the Oxford® mobile partial knee implant were analyzed between July 2014 and September 2022. Various preoperative and postoperative radiographic parameters determining pre- and postoperative alignment and implant positioning, incidence and characteristics of periprosthetic fractures, and patient demographics were assessed. Statistical analyses, including Mann-Whitney U test and logistic regression, were conducted to identify significant associations and predictors of tibial fractures.</p><p><strong>Results: </strong>Of the 1853 cases that were finally included in the study, 19 (1%) patients experienced TPF. The fracture group presented with a significantly shorter relative mediolateral and posteroanterior distance between the keel and cortex [mediolateral: 23.3% (23.2-24.8%) versus 27.1% (25.7-28.3%), p < 0.001; posteroanterior: 8.4% (6.3-10.3%) versus 10.0% (9.8-10.1%), p = 0.004]. Additionally, an increased posterior tibial slope in pre- and postoperative radiographs [preoperative: 10.4° (8.6-11.1°) versus 7.7° (5.4-10.0°), p < 0.001; postoperative 9.1° ± 3.1° versus 7.5° (5.9-9.0°), p = 0.030] was observed in the fracture group. Furthermore, the use of smaller-sized implants (AA) was associated with higher fracture rates (p < 0.001). Anatomical variants, such as a medial overhanging tibial plateau, were not observed.</p><p><strong>Conclusions: </strong>In UKA, type Oxford TPF are linked to shorter mediolateral and posteroanterior keel-cortex distances, increased pre- and postoperative PTS, and small implant sizes (AA). Fracture lines often extend from the distal keel to the medial tibial cortex. These findings emphasize the importance of precise implant positioning and sizing to minimize fracture risk. Level of evidence Retrospective single-center study, III.</p>","PeriodicalId":36317,"journal":{"name":"Knee Surgery and Related Research","volume":"36 1","pages":"36"},"PeriodicalIF":4.4000,"publicationDate":"2024-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11583789/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Knee Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s43019-024-00237-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: This retrospective single-center study aimed to investigate incidence and risk factors influencing tibial periprosthetic fractures (TPF) in Oxford unicompartmental knee arthroplasty (UKA), with a specific focus on tibial component positioning and sizing.
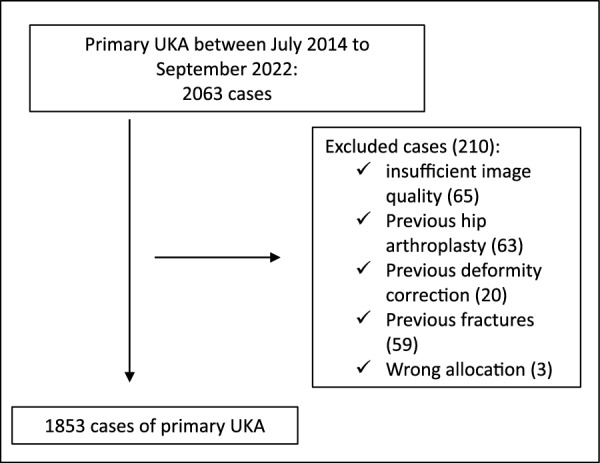
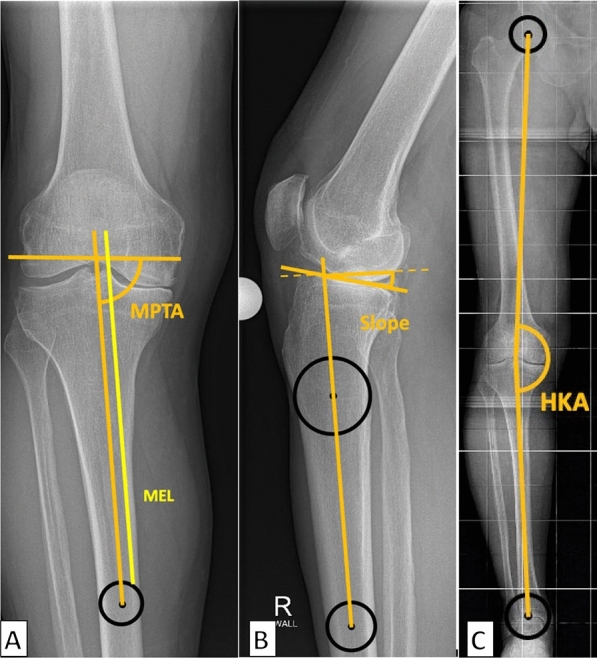
Methods: A total of 2063 patients with medial UKA using the Oxford® mobile partial knee implant were analyzed between July 2014 and September 2022. Various preoperative and postoperative radiographic parameters determining pre- and postoperative alignment and implant positioning, incidence and characteristics of periprosthetic fractures, and patient demographics were assessed. Statistical analyses, including Mann-Whitney U test and logistic regression, were conducted to identify significant associations and predictors of tibial fractures.
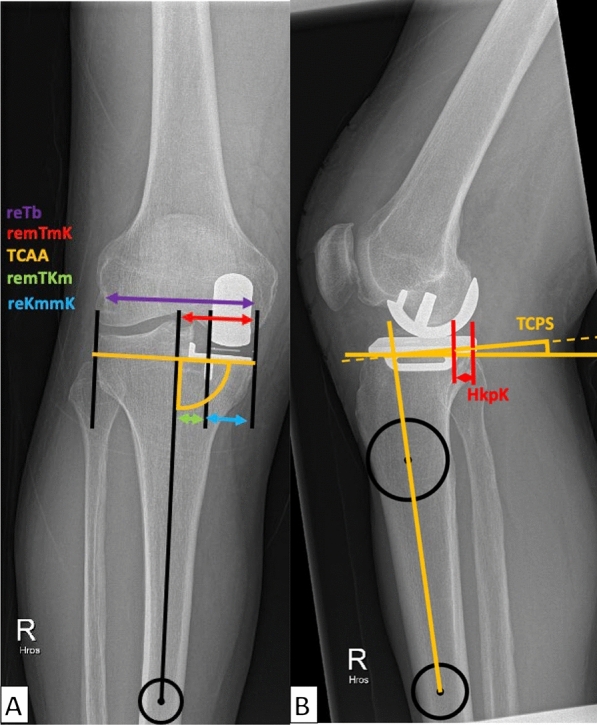
Results: Of the 1853 cases that were finally included in the study, 19 (1%) patients experienced TPF. The fracture group presented with a significantly shorter relative mediolateral and posteroanterior distance between the keel and cortex [mediolateral: 23.3% (23.2-24.8%) versus 27.1% (25.7-28.3%), p < 0.001; posteroanterior: 8.4% (6.3-10.3%) versus 10.0% (9.8-10.1%), p = 0.004]. Additionally, an increased posterior tibial slope in pre- and postoperative radiographs [preoperative: 10.4° (8.6-11.1°) versus 7.7° (5.4-10.0°), p < 0.001; postoperative 9.1° ± 3.1° versus 7.5° (5.9-9.0°), p = 0.030] was observed in the fracture group. Furthermore, the use of smaller-sized implants (AA) was associated with higher fracture rates (p < 0.001). Anatomical variants, such as a medial overhanging tibial plateau, were not observed.
Conclusions: In UKA, type Oxford TPF are linked to shorter mediolateral and posteroanterior keel-cortex distances, increased pre- and postoperative PTS, and small implant sizes (AA). Fracture lines often extend from the distal keel to the medial tibial cortex. These findings emphasize the importance of precise implant positioning and sizing to minimize fracture risk. Level of evidence Retrospective single-center study, III.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
