{"title":"Time-dependent improvements in pacing thresholds with lumenless leads placed in the right atrium","authors":"Yasumasa Nohno MD , Ryosuke Kozu MD , Shusaku Maruyama MD , Tomoya Hasegawa MD , Hiromi Tsuchiya MD , Takahiro Tachibana MD , Hikaru Kimura MD , Yoshikazu Yazaki MD, PhD , Katsuhito Fujiu MD, PhD","doi":"10.1016/j.hroo.2024.09.009","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Traditional pacemaker implantation often poses risks, such as perforation when positioning atrial leads at the right atrial appendage (RAA). Recent advancements in delivery catheters have enabled atrial lead placement in the right atrial septum, potentially mitigating RAA-related complications. However, the performance of lumenless leads in this context remains unclear.</div></div><div><h3>Objective</h3><div>This study was performed to assess the performance of lumenless leads as atrial leads.</div></div><div><h3>Methods</h3><div>Forty-four consecutive patients undergoing pacemaker implantation with lumenless atrial leads were enrolled. Lead implantation was performed using a 3830 SelectSecure lead and C315HIS-sheath. Pacing parameters were collected immediately after screwing, 3 and 5 minutes later, at the end of the procedure, and at every 6-month follow-up.</div></div><div><h3>Results</h3><div>Lead parameters including P-wave, pacing threshold, and impedance significantly improved over time. The threshold levels from 2.00 ± 0.72 V/0.4 msec immediately after screwing to 1.45 ± 0.57 V/0.4 msec at 5 minutes, 0.95 ± 0.38 V/0.4 msec at the end of the procedure, and 0.78 ± 0.39 V/0.4 msec at discharge. Initially, threshold levels were >2.5 V/0.4 msec in 15 cases; however, they decreased to <2 V/0.4 msec by the end of the procedure. At discharge, 13 of the 15 cases showed a threshold decrease to <1 V/0.4 msec. During follow-up, no threshold increase (>1 V), lead revision, or battery depletion was observed.</div></div><div><h3>Conclusion</h3><div>Lumenless lead placement in the right atrium results in threshold decrease over time. Therefore, allowing a waiting period instead of immediately repositioning the lead may be more effective when thresholds are high after screwing.</div></div>","PeriodicalId":29772,"journal":{"name":"Heart Rhythm O2","volume":"5 11","pages":"Pages 764-769"},"PeriodicalIF":2.9000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Heart Rhythm O2","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666501824003003","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/20 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Traditional pacemaker implantation often poses risks, such as perforation when positioning atrial leads at the right atrial appendage (RAA). Recent advancements in delivery catheters have enabled atrial lead placement in the right atrial septum, potentially mitigating RAA-related complications. However, the performance of lumenless leads in this context remains unclear.
Objective
This study was performed to assess the performance of lumenless leads as atrial leads.
Methods
Forty-four consecutive patients undergoing pacemaker implantation with lumenless atrial leads were enrolled. Lead implantation was performed using a 3830 SelectSecure lead and C315HIS-sheath. Pacing parameters were collected immediately after screwing, 3 and 5 minutes later, at the end of the procedure, and at every 6-month follow-up.
Results
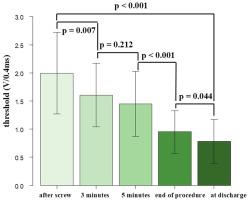
Lead parameters including P-wave, pacing threshold, and impedance significantly improved over time. The threshold levels from 2.00 ± 0.72 V/0.4 msec immediately after screwing to 1.45 ± 0.57 V/0.4 msec at 5 minutes, 0.95 ± 0.38 V/0.4 msec at the end of the procedure, and 0.78 ± 0.39 V/0.4 msec at discharge. Initially, threshold levels were >2.5 V/0.4 msec in 15 cases; however, they decreased to <2 V/0.4 msec by the end of the procedure. At discharge, 13 of the 15 cases showed a threshold decrease to <1 V/0.4 msec. During follow-up, no threshold increase (>1 V), lead revision, or battery depletion was observed.
Conclusion
Lumenless lead placement in the right atrium results in threshold decrease over time. Therefore, allowing a waiting period instead of immediately repositioning the lead may be more effective when thresholds are high after screwing.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
