Rongrong Bian, Feng Zhao, Bo Peng, Jin Zhang, Qixing Mao, Lin Wang, Qiang Chen
{"title":"A Nomogram for Predicting Recurrence in Stage I Non-Small Cell Lung Cancer","authors":"Rongrong Bian, Feng Zhao, Bo Peng, Jin Zhang, Qixing Mao, Lin Wang, Qiang Chen","doi":"10.1111/crj.70022","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Early-stage non–small cell lung cancer (NSCLC) is being diagnosed increasingly, and in 30% of diagnosed patients, recurrence will develop within 5 years. Thus, it is urgent to identify recurrence-related markers to optimize the management of patient-tailored therapeutics.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>The eligible datasets were downloaded from TCGA and GEO. In the discovery phase, two algorithms, least absolute shrinkage and selector operation and support vector machine-recursive feature elimination, were used to identify candidate genes. The recurrence-associated signature was developed by penalized Cox regression. The nomogram was constructed and further tested via other independent cohorts.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>In this retrospective study, 14 eligible datasets and 7 published signatures were included. A 13-gene based signature was generated by penalized Cox regression categorized training cohort into high-risk and low-risk subgroups (HR = 8.873, 95% CI: 4.228–18.480 <i>p</i> < 0.001). Furthermore, a nomogram integrating the recurrence-related signature, age, and histology was developed to predict the recurrence-free survival in the training cohort, which performed well in the two external validation cohorts (concordance index: 0.737, 95% CI: 0.732–0.742, <i>p</i> < 0.001; 0.666, 95% CI: 0.650–0.682, <i>p</i> < 0.001; 0.651, 95% CI: 0.637–0.665, <i>p</i> < 0.001, respectively). The nomogram was further performed well in the Jiangsu cohort enrolled 163 patients (HR = 2.723, 95% CI: 1.526–4.859, <i>p</i> = 0.001). Post-operative adjuvant therapy achieved evaluated disease-free survival in high and intermediate risk groups (HR = 4.791, 95% CI: 1.081–21.231, <i>p</i> = 0.039).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>The proposed nomogram is a promising tool for estimating recurrence-free survival in stage I NSCLC, which might have tremendous value in management of early stage NSCLC and guiding adjuvant therapy strategies.</p>\n </section>\n </div>","PeriodicalId":55247,"journal":{"name":"Clinical Respiratory Journal","volume":"18 11","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2024-11-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/crj.70022","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Respiratory Journal","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/crj.70022","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Early-stage non–small cell lung cancer (NSCLC) is being diagnosed increasingly, and in 30% of diagnosed patients, recurrence will develop within 5 years. Thus, it is urgent to identify recurrence-related markers to optimize the management of patient-tailored therapeutics.
Methods
The eligible datasets were downloaded from TCGA and GEO. In the discovery phase, two algorithms, least absolute shrinkage and selector operation and support vector machine-recursive feature elimination, were used to identify candidate genes. The recurrence-associated signature was developed by penalized Cox regression. The nomogram was constructed and further tested via other independent cohorts.
Results
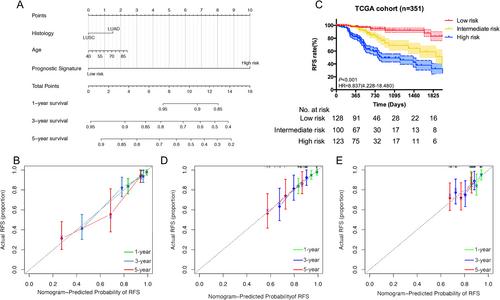
In this retrospective study, 14 eligible datasets and 7 published signatures were included. A 13-gene based signature was generated by penalized Cox regression categorized training cohort into high-risk and low-risk subgroups (HR = 8.873, 95% CI: 4.228–18.480 p < 0.001). Furthermore, a nomogram integrating the recurrence-related signature, age, and histology was developed to predict the recurrence-free survival in the training cohort, which performed well in the two external validation cohorts (concordance index: 0.737, 95% CI: 0.732–0.742, p < 0.001; 0.666, 95% CI: 0.650–0.682, p < 0.001; 0.651, 95% CI: 0.637–0.665, p < 0.001, respectively). The nomogram was further performed well in the Jiangsu cohort enrolled 163 patients (HR = 2.723, 95% CI: 1.526–4.859, p = 0.001). Post-operative adjuvant therapy achieved evaluated disease-free survival in high and intermediate risk groups (HR = 4.791, 95% CI: 1.081–21.231, p = 0.039).
Conclusions
The proposed nomogram is a promising tool for estimating recurrence-free survival in stage I NSCLC, which might have tremendous value in management of early stage NSCLC and guiding adjuvant therapy strategies.
期刊介绍:
Overview
Effective with the 2016 volume, this journal will be published in an online-only format.
Aims and Scope
The Clinical Respiratory Journal (CRJ) provides a forum for clinical research in all areas of respiratory medicine from clinical lung disease to basic research relevant to the clinic.
We publish original research, review articles, case studies, editorials and book reviews in all areas of clinical lung disease including:
Asthma
Allergy
COPD
Non-invasive ventilation
Sleep related breathing disorders
Interstitial lung diseases
Lung cancer
Clinical genetics
Rhinitis
Airway and lung infection
Epidemiology
Pediatrics
CRJ provides a fast-track service for selected Phase II and Phase III trial studies.
Keywords
Clinical Respiratory Journal, respiratory, pulmonary, medicine, clinical, lung disease,
Abstracting and Indexing Information
Academic Search (EBSCO Publishing)
Academic Search Alumni Edition (EBSCO Publishing)
Embase (Elsevier)
Health & Medical Collection (ProQuest)
Health Research Premium Collection (ProQuest)
HEED: Health Economic Evaluations Database (Wiley-Blackwell)
Hospital Premium Collection (ProQuest)
Journal Citation Reports/Science Edition (Clarivate Analytics)
MEDLINE/PubMed (NLM)
ProQuest Central (ProQuest)
Science Citation Index Expanded (Clarivate Analytics)
SCOPUS (Elsevier)



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
