Panthea Pouramin, Susan E Allen, Joseph L Silburt, Boris L Gala-Lopez
{"title":"Median Meld at Transplant Minus 3 Reduces the Mortality of Non-Hepatocellular Carcinoma Patients on the Liver Transplant Waitlist.","authors":"Panthea Pouramin, Susan E Allen, Joseph L Silburt, Boris L Gala-Lopez","doi":"10.3390/curroncol31110519","DOIUrl":null,"url":null,"abstract":"<p><p>Liver transplants (LTs) are prioritized by mortality risk, which is estimated by MELD scores. Since hepatocellular carcinoma (HCC) patients present with lower MELD scores, they are allocated MELD exception points. Concerns persist that HCC recipients are over-prioritized, resulting in disproportionate waitlist mortality among non-HCC patients. We assessed whether the Median Meld at Transplant minus 3 (MMaT-3) scoring system would balance waitlist mortality and transplantation rates between HCC and non-HCC patients. We reviewed 266 patient charts listed for an LT from 2015 to 2023; 46.2% were listed in the MMaT-3 era. Amongst non-HCC patients, MMaT-3 implementation significantly increased 1-year transplant rate and reduced 1-year waitlist mortality among non-HCC patients (<i>p</i> = 0.003). Pre-MMaT-3 gaps in transplantation (<i>p</i> = 0.004) and waitlist dropout (<i>p</i> = 0.01) were eliminated post-implementation (<i>p</i> > 0.05). Amongst HCC patients, MMaT-3 implementation had no impact on the 1-year transplant rate (<i>p</i> = 0.92) or 1-year waitlist mortality (<i>p</i> = 0.66). Fine-gray proportional hazard multivariable analysis revealed that MMaT-3 significantly reduced waitlist mortality among non-HCC patients (asHR: 0.44, 95% CI [0.23, 0.83], <i>p</i> = 0.01) and limited impact on HCC patients (<i>p</i> = 0.31). MMaT-3 allocation did not significantly alter 2-year post-transplant survival for both populations. We show that the MMaT-3 system decreased the waitlist mortality of non-HCC patients with limited impacts on outcomes for HCC patients listed for an LT.</p>","PeriodicalId":11012,"journal":{"name":"Current oncology","volume":"31 11","pages":"7051-7060"},"PeriodicalIF":3.4000,"publicationDate":"2024-11-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11592907/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/curroncol31110519","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
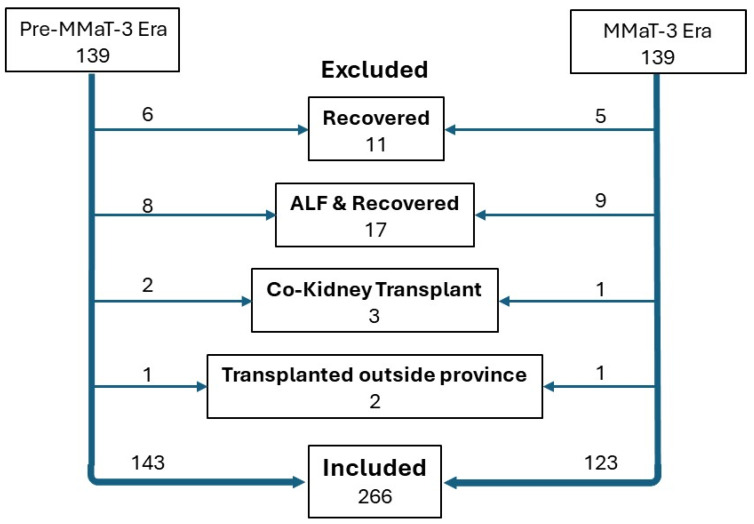
Liver transplants (LTs) are prioritized by mortality risk, which is estimated by MELD scores. Since hepatocellular carcinoma (HCC) patients present with lower MELD scores, they are allocated MELD exception points. Concerns persist that HCC recipients are over-prioritized, resulting in disproportionate waitlist mortality among non-HCC patients. We assessed whether the Median Meld at Transplant minus 3 (MMaT-3) scoring system would balance waitlist mortality and transplantation rates between HCC and non-HCC patients. We reviewed 266 patient charts listed for an LT from 2015 to 2023; 46.2% were listed in the MMaT-3 era. Amongst non-HCC patients, MMaT-3 implementation significantly increased 1-year transplant rate and reduced 1-year waitlist mortality among non-HCC patients (p = 0.003). Pre-MMaT-3 gaps in transplantation (p = 0.004) and waitlist dropout (p = 0.01) were eliminated post-implementation (p > 0.05). Amongst HCC patients, MMaT-3 implementation had no impact on the 1-year transplant rate (p = 0.92) or 1-year waitlist mortality (p = 0.66). Fine-gray proportional hazard multivariable analysis revealed that MMaT-3 significantly reduced waitlist mortality among non-HCC patients (asHR: 0.44, 95% CI [0.23, 0.83], p = 0.01) and limited impact on HCC patients (p = 0.31). MMaT-3 allocation did not significantly alter 2-year post-transplant survival for both populations. We show that the MMaT-3 system decreased the waitlist mortality of non-HCC patients with limited impacts on outcomes for HCC patients listed for an LT.
期刊介绍:
Current Oncology is a peer-reviewed, Canadian-based and internationally respected journal. Current Oncology represents a multidisciplinary medium encompassing health care workers in the field of cancer therapy in Canada to report upon and to review progress in the management of this disease.
We encourage submissions from all fields of cancer medicine, including radiation oncology, surgical oncology, medical oncology, pediatric oncology, pathology, and cancer rehabilitation and survivorship. Articles published in the journal typically contain information that is relevant directly to clinical oncology practice, and have clear potential for application to the current or future practice of cancer medicine.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
