Hospital readmissions following catheter ablation for atrial fibrillation with THERMOCOOL™ STSF/ THERMOCOOL™ ST catheter with CARTO™ 3 system versus TactiCath™ catheter with EnSite™ system.
Alexandru I Costea, Rahul Khanna, Maximiliano Iglesias, Yiran Rong
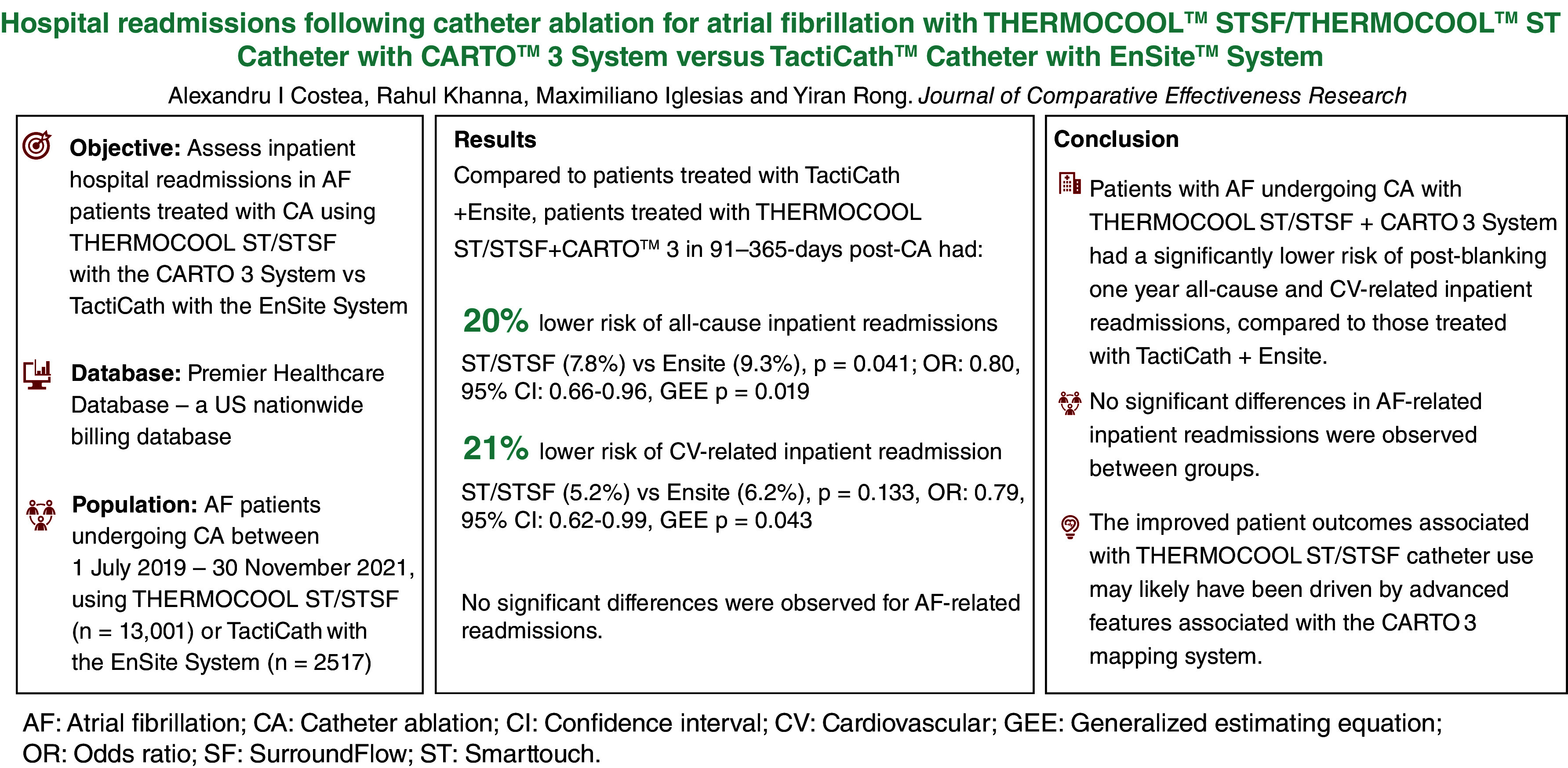
{"title":"Hospital readmissions following catheter ablation for atrial fibrillation with THERMOCOOL™ STSF/ THERMOCOOL™ ST catheter with CARTO™ 3 system versus TactiCath™ catheter with EnSite™ system.","authors":"Alexandru I Costea, Rahul Khanna, Maximiliano Iglesias, Yiran Rong","doi":"10.57264/cer-2024-0075","DOIUrl":null,"url":null,"abstract":"<p><p><b>Aim:</b> Radiofrequency (RF) catheter ablation (CA) is a mainstay treatment for atrial fibrillation (AF). RF catheters with contact force (CF) sensing technology and electroanatomical mapping systems enable real-time assessment of catheter tip-tissue interface CF, facilitating individualized and precise CA. This study examined inpatient hospital readmissions in patients with AF treated with THERMOCOOL™ ST/ THERMOCOOL™ STSF catheter with the CARTO™ 3 System versus TactiCath™ catheter with the EnSite™ System. <b>Materials</b> <b>&</b> <b>methods:</b> Patients undergoing CA for AF between 1 July 2019 to 30 November 2021 were identified from the Premier Healthcare Database and grouped based on use of THERMOCOOL ST/STSF or TactiCath™. Study outcomes were all-cause, cardiovascular (CV)-, and AF-related inpatient readmission at 91-365-day post-CA. Inverse probability of treatment weighting of propensity scores balanced baseline patient, comorbidity and hospital characteristics. A weighted generalized estimating equation (GEE) model examined differences in readmission outcomes. <b>Results:</b> A total of 15,518 patients met inclusion criteria (THERMOCOOL ST/STSF, n = 13,001; TactiCath™, n = 2517). Patient characteristics were generally well-balanced after weighting. Patients treated with THERMOCOOL ST/STSF + CARTO 3 had a 20% lower likelihood of all-cause inpatient readmissions (7.8 vs 9.3%, chi-square p = 0.041; odds ratio [OR]: 0.80, 95% confidence interval [CI]: 0.66-0.96, GEE p = 0.019) and a 21% lower likelihood of CV-related inpatient readmission (5.2 vs 6.2%, chi-square p = 0.133, OR: 0.79, 95% CI: 0.62-0.99, GEE p = 0.043) in 91-365-days post-CA versus those treated with TactiCath™ + Ensite. No significant differences were observed for AF-related readmissions. <b>Conclusion:</b> Patients undergoing CA for AF treated with THERMOCOOL ST/STSF + CARTO 3 had a significantly lower risk of all-cause and CV-related inpatient hospital readmission versus those treated with TactiCath™ + Ensite.</p>","PeriodicalId":15539,"journal":{"name":"Journal of comparative effectiveness research","volume":" ","pages":"e240075"},"PeriodicalIF":2.5000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11656344/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of comparative effectiveness research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.57264/cer-2024-0075","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/4 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: Radiofrequency (RF) catheter ablation (CA) is a mainstay treatment for atrial fibrillation (AF). RF catheters with contact force (CF) sensing technology and electroanatomical mapping systems enable real-time assessment of catheter tip-tissue interface CF, facilitating individualized and precise CA. This study examined inpatient hospital readmissions in patients with AF treated with THERMOCOOL™ ST/ THERMOCOOL™ STSF catheter with the CARTO™ 3 System versus TactiCath™ catheter with the EnSite™ System. Materials&methods: Patients undergoing CA for AF between 1 July 2019 to 30 November 2021 were identified from the Premier Healthcare Database and grouped based on use of THERMOCOOL ST/STSF or TactiCath™. Study outcomes were all-cause, cardiovascular (CV)-, and AF-related inpatient readmission at 91-365-day post-CA. Inverse probability of treatment weighting of propensity scores balanced baseline patient, comorbidity and hospital characteristics. A weighted generalized estimating equation (GEE) model examined differences in readmission outcomes. Results: A total of 15,518 patients met inclusion criteria (THERMOCOOL ST/STSF, n = 13,001; TactiCath™, n = 2517). Patient characteristics were generally well-balanced after weighting. Patients treated with THERMOCOOL ST/STSF + CARTO 3 had a 20% lower likelihood of all-cause inpatient readmissions (7.8 vs 9.3%, chi-square p = 0.041; odds ratio [OR]: 0.80, 95% confidence interval [CI]: 0.66-0.96, GEE p = 0.019) and a 21% lower likelihood of CV-related inpatient readmission (5.2 vs 6.2%, chi-square p = 0.133, OR: 0.79, 95% CI: 0.62-0.99, GEE p = 0.043) in 91-365-days post-CA versus those treated with TactiCath™ + Ensite. No significant differences were observed for AF-related readmissions. Conclusion: Patients undergoing CA for AF treated with THERMOCOOL ST/STSF + CARTO 3 had a significantly lower risk of all-cause and CV-related inpatient hospital readmission versus those treated with TactiCath™ + Ensite.
期刊介绍:
Journal of Comparative Effectiveness Research provides a rapid-publication platform for debate, and for the presentation of new findings and research methodologies.
Through rigorous evaluation and comprehensive coverage, the Journal of Comparative Effectiveness Research provides stakeholders (including patients, clinicians, healthcare purchasers, and health policy makers) with the key data and opinions to make informed and specific decisions on clinical practice.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
