Clinical and economic implications of focal dissection treatment following percutaneous transluminal angioplasty of the superficial femoral artery: an exploratory analysis based on the TOBA II Study.
Jan B Pietzsch, Benjamin P Geisler, Abigail M Garner, Anne M Ryschon, William A Gray, Masahiko Fujihara, Peter A Schneider
{"title":"Clinical and economic implications of focal dissection treatment following percutaneous transluminal angioplasty of the superficial femoral artery: an exploratory analysis based on the TOBA II Study.","authors":"Jan B Pietzsch, Benjamin P Geisler, Abigail M Garner, Anne M Ryschon, William A Gray, Masahiko Fujihara, Peter A Schneider","doi":"10.57264/cer-2024-0055","DOIUrl":null,"url":null,"abstract":"<p><p><b>Aim:</b> Percutaneous transluminal angioplasty (PTA) for peripheral artery disease (PAD) commonly leads to dissections which are associated with higher target lesion revascularization (TLR) rates. Clinical and economic consequences of dissection management in the femoropopliteal artery following PTA, and specifically the potential economic benefit of focal dissection repair using the novel Tack Endovascular System, remain unknown. <b>Methods:</b> A decision-analytic model was used to estimate 24-month clinical events, costs and quality-adjusted life year (QALY) gain for a Tack-supported versus status-quo PTA strategy. Patient and lesion characteristics and TLR rates were derived from the PTA cohort of the TOBA II clinical trial, an observational cohort, and literature. Cost-effectiveness was determined from a US payer and provider perspective separately for the non-severe (grade A or B), severe (grade C and higher) and the entire dissection cohort. <b>Results:</b> TLR rates were lower for the Tack-supported strategy compared with PTA (7.7 vs 27.4% in the non-severe, 13.9 vs 25.8% in the severe and 12.0 vs 26.3% in the entire dissection cohort). Cost and QALY differences were +$297/ + 0.0110 in the non-severe dissection cohort and -$1602/ + 0.0067 in the severe dissection cohort, resulting in an incremental cost-effectiveness ratio (ICER) of $25,622 in the non-severe cohort and dominance in the severe cohort and the entire cohort. <b>Conclusion:</b> Compared with a 'status-quo' approach, proactive focal stenting may lead to fewer reinterventions and improved quality of life. There appears to be a graded economic benefit of focal dissection treatment, being cost-effective in non-severe dissections and even cost saving in severe dissections.</p>","PeriodicalId":15539,"journal":{"name":"Journal of comparative effectiveness research","volume":" ","pages":"e240055"},"PeriodicalIF":2.5000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11656342/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of comparative effectiveness research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.57264/cer-2024-0055","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/2 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
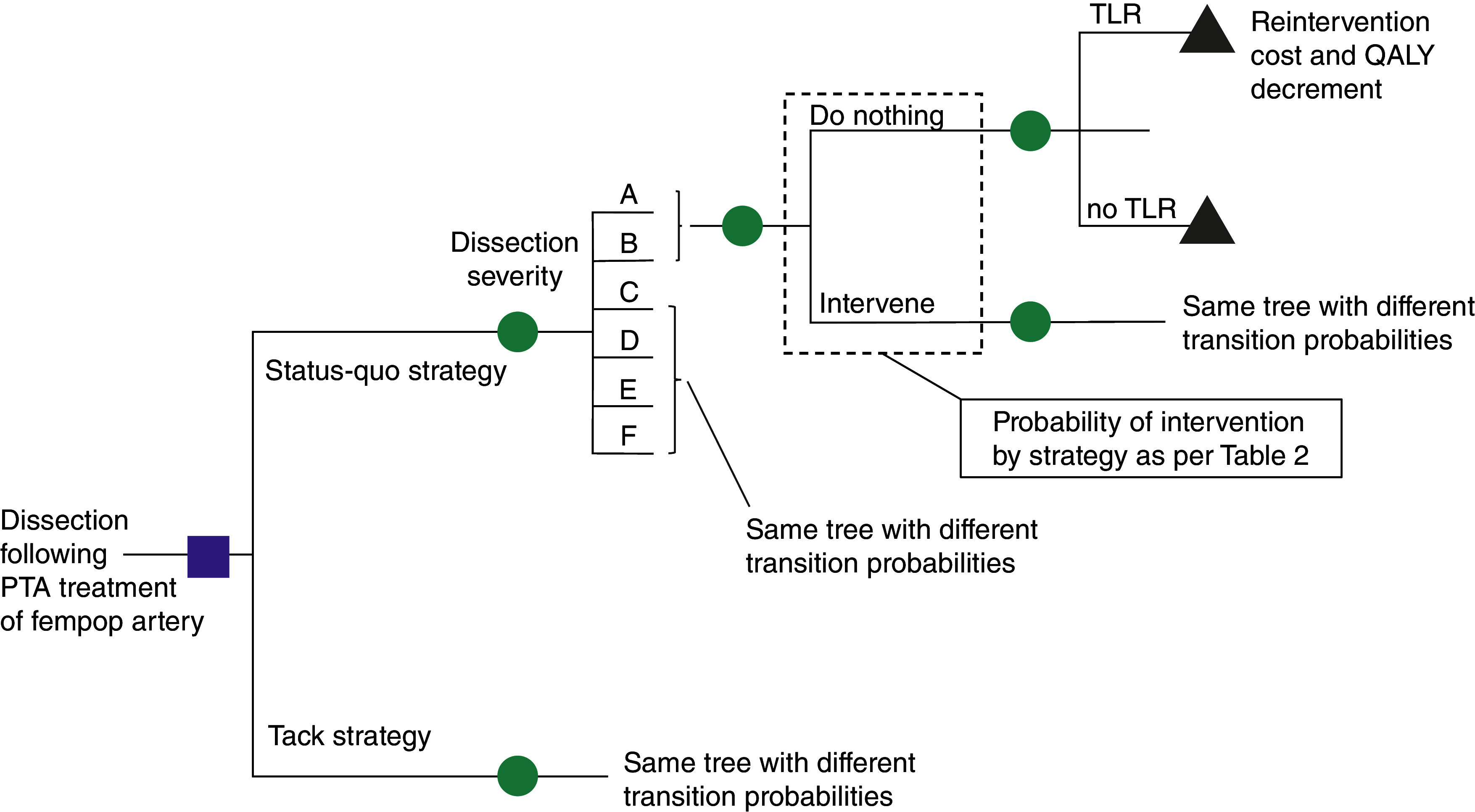
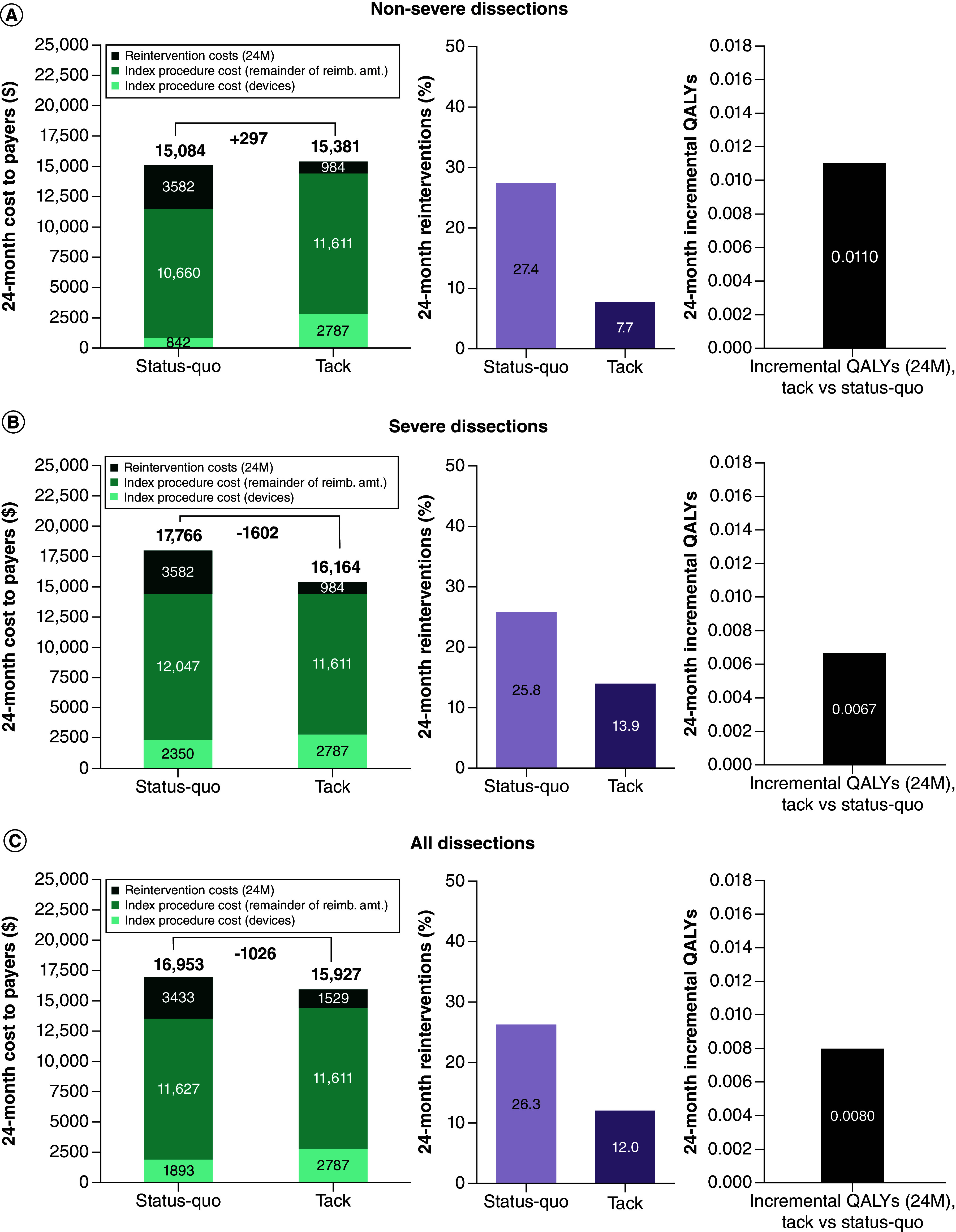
Aim: Percutaneous transluminal angioplasty (PTA) for peripheral artery disease (PAD) commonly leads to dissections which are associated with higher target lesion revascularization (TLR) rates. Clinical and economic consequences of dissection management in the femoropopliteal artery following PTA, and specifically the potential economic benefit of focal dissection repair using the novel Tack Endovascular System, remain unknown. Methods: A decision-analytic model was used to estimate 24-month clinical events, costs and quality-adjusted life year (QALY) gain for a Tack-supported versus status-quo PTA strategy. Patient and lesion characteristics and TLR rates were derived from the PTA cohort of the TOBA II clinical trial, an observational cohort, and literature. Cost-effectiveness was determined from a US payer and provider perspective separately for the non-severe (grade A or B), severe (grade C and higher) and the entire dissection cohort. Results: TLR rates were lower for the Tack-supported strategy compared with PTA (7.7 vs 27.4% in the non-severe, 13.9 vs 25.8% in the severe and 12.0 vs 26.3% in the entire dissection cohort). Cost and QALY differences were +$297/ + 0.0110 in the non-severe dissection cohort and -$1602/ + 0.0067 in the severe dissection cohort, resulting in an incremental cost-effectiveness ratio (ICER) of $25,622 in the non-severe cohort and dominance in the severe cohort and the entire cohort. Conclusion: Compared with a 'status-quo' approach, proactive focal stenting may lead to fewer reinterventions and improved quality of life. There appears to be a graded economic benefit of focal dissection treatment, being cost-effective in non-severe dissections and even cost saving in severe dissections.
目的:外周动脉疾病(PAD)的经皮腔内血管成形术(PTA)通常导致夹层,并伴有较高的靶病变血运重建率。PTA术后股腘动脉夹层处理的临床和经济后果,特别是使用新型Tack血管内系统进行局灶性夹层修复的潜在经济效益尚不清楚。方法:采用决策分析模型来评估治疗支持与现状PTA策略的24个月临床事件、成本和质量调整生命年(QALY)增益。患者和病变特征以及TLR率来源于TOBA II临床试验的PTA队列、观察队列和文献。成本效益分别从美国支付者和提供者的角度确定非严重(a级或B级)、严重(C级及以上)和整个夹层队列。结果:与PTA相比,tac支持策略的TLR率较低(非严重组为7.7 vs 27.4%,严重组为13.9 vs 25.8%,整个夹层队列为12.0 vs 26.3%)。成本和质量差异在非严重夹层队列中为+ 297美元/ + 0.0110美元,在严重夹层队列中为- 1602美元/ + 0.0067美元,导致非严重夹层队列的增量成本-效果比(ICER)为25,622美元,在严重夹层队列和整个队列中占主导地位。结论:与“现状”方法相比,主动局灶支架置入可减少再干预并改善生活质量。局灶性解剖治疗似乎具有分级的经济效益,在非严重解剖中具有成本效益,甚至在严重解剖中节省成本。
期刊介绍:
Journal of Comparative Effectiveness Research provides a rapid-publication platform for debate, and for the presentation of new findings and research methodologies.
Through rigorous evaluation and comprehensive coverage, the Journal of Comparative Effectiveness Research provides stakeholders (including patients, clinicians, healthcare purchasers, and health policy makers) with the key data and opinions to make informed and specific decisions on clinical practice.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
