Peter Calvert, Mark T Mills, Ben Murray, Jonathan Kendall, Justin Ratnasingham, Vishal Luther, Dhiraj Gupta
{"title":"Feasibility of pulsed field ablation for atrial fibrillation under mild conscious sedation.","authors":"Peter Calvert, Mark T Mills, Ben Murray, Jonathan Kendall, Justin Ratnasingham, Vishal Luther, Dhiraj Gupta","doi":"10.1007/s10840-024-01961-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pulsed field ablation (PFA) is a new modality for pulmonary vein isolation (PVI) for atrial fibrillation (AF). PFA is performed under general anaesthetic (GA) or deep sedation with propofol, but this requires anaesthetic support in many countries, restricting use. No study has tested the feasibility of PFA under mild conscious sedation (MCS).</p><p><strong>Methods: </strong>We prospectively recruited patients undergoing PFA PVI, offered the option of MCS delivered by electrophysiologists, and compared these with patients who opted for GA. MCS comprised intravenous midazolam and fentanyl. All procedures were performed under anaesthetic supervision in case of requirement to convert to GA, which formed the primary outcome.</p><p><strong>Results: </strong>Twenty-three patients were recruited (8 MCS, 15 GA). One patient (1/8 [12.5%]) required conversion from MCS to GA. Total procedural times were similar between groups (MCS 92 ± 12.4 min vs. GA 101 ± 17.3 min; p = 0.199). High mean sedative doses were required in the MCS group (5.12 ± 0.83 mg midazolam and 209 ± 40 mcg fentanyl). Median intraprocedural pain perception by the patient, rated from 0 to 100 was 45 (IQR 22.5-72.5) in the MCS group. Post-procedural groin pain (0 [0-0] vs. 5 [0-35]; p = 0.027) and throat pain (0 [0-0] vs. 10 [5-40]; p = 0.001) were lower in the MCS group.</p><p><strong>Conclusion: </strong>PFA under MCS is feasible in selected patients but pain and tolerance may be suboptimal, and high sedative doses are required.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"1429-1436"},"PeriodicalIF":2.6000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436502/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-024-01961-1","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/2 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
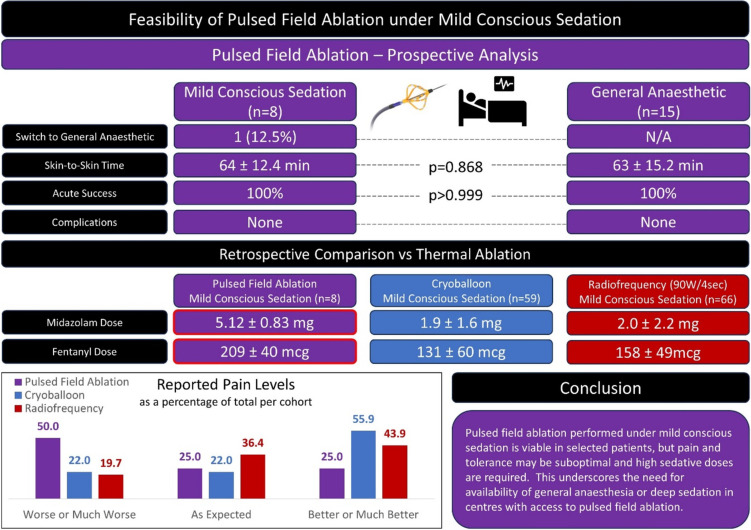
Background: Pulsed field ablation (PFA) is a new modality for pulmonary vein isolation (PVI) for atrial fibrillation (AF). PFA is performed under general anaesthetic (GA) or deep sedation with propofol, but this requires anaesthetic support in many countries, restricting use. No study has tested the feasibility of PFA under mild conscious sedation (MCS).
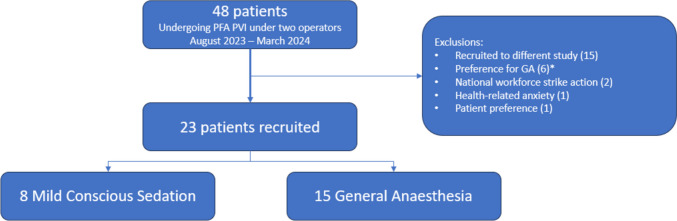
Methods: We prospectively recruited patients undergoing PFA PVI, offered the option of MCS delivered by electrophysiologists, and compared these with patients who opted for GA. MCS comprised intravenous midazolam and fentanyl. All procedures were performed under anaesthetic supervision in case of requirement to convert to GA, which formed the primary outcome.
Results: Twenty-three patients were recruited (8 MCS, 15 GA). One patient (1/8 [12.5%]) required conversion from MCS to GA. Total procedural times were similar between groups (MCS 92 ± 12.4 min vs. GA 101 ± 17.3 min; p = 0.199). High mean sedative doses were required in the MCS group (5.12 ± 0.83 mg midazolam and 209 ± 40 mcg fentanyl). Median intraprocedural pain perception by the patient, rated from 0 to 100 was 45 (IQR 22.5-72.5) in the MCS group. Post-procedural groin pain (0 [0-0] vs. 5 [0-35]; p = 0.027) and throat pain (0 [0-0] vs. 10 [5-40]; p = 0.001) were lower in the MCS group.
Conclusion: PFA under MCS is feasible in selected patients but pain and tolerance may be suboptimal, and high sedative doses are required.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
