{"title":"Perioperative Blood Pressure Management Recommendations in Pediatric Pheochromocytoma: A 10-Year Narrative Review.","authors":"Cahyani Gita Ambarsari, Nadhifah Nadhifah, Hertanti Indah Lestari","doi":"10.1159/000542897","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pheochromocytomas and paragangliomas are rare chromaffin cell-derived tumors characterized by catecholamine-secreting activity. Pheochromocytomas account for 1.7% of pediatric hypertension cases. Surgical resection, the definitive pheochromocytoma treatment, carries risks of hemodynamic instability and cardiovascular complications. Nevertheless, mortality rates decreased significantly in the latter half of the 20th century due to effective perioperative blood pressure (BP) management. The literature on BP management tailored to pediatric pheochromocytoma is limited, while the sustained hypertension rate in this population is high (up to 90%) and related to a high risk of intraoperative complications. In this narrative review, we provide up-to-date recommendations regarding BP management to minimize perioperative comorbidities in children with pheochromocytoma.</p><p><strong>Summary: </strong>Antihypertensive agents, primarily alpha (α)-blockers, should be promptly administered for suspected pheochromocytoma. Beta (β)-blockers may be introduced thereafter to counteract reflex tachycardia. The patient must be salt- and water-replete preoperation. Intraoperatively, stable hemodynamics should be ensured during anesthesia and surgery, and short-acting intravenous medications and resuscitation fluid should be supplied. Postoperatively, patients should be admitted to the pediatric intensive care unit for close monitoring for at least 24-48 h. Genetic testing is recommended for all pheochromocytoma patients. Identifying underlying mutations, like in succinate dehydrogenase subunit B, which is linked to a higher risk of multifocality and metastasis, is imperative for tailoring treatment strategies and prognostication.</p><p><strong>Key messages: </strong>Achieving optimal outcomes in pediatric pheochromocytoma relies on preoperative BP optimization with appropriate antihypertensive agents, intraoperative hemodynamic stability, and postoperative routine long-term follow-up to monitor for complications, recurrence, and metastasis. Future research should prioritize well-designed prospective multicenter studies with adequate sample sizes and, where feasible, randomized controlled trials with standardized protocols and appropriate endpoints. These studies should focus on the efficacy and safety of preoperative nonselective versus selective α-blockers, whether as monotherapy or combined with other medications (e.g., calcium channel blockers and/or β-blockers), or treatment without preoperative anti-hypertensives.</p>","PeriodicalId":17813,"journal":{"name":"Kidney & blood pressure research","volume":" ","pages":"61-82"},"PeriodicalIF":2.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11844699/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kidney & blood pressure research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000542897","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/3 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pheochromocytomas and paragangliomas are rare chromaffin cell-derived tumors characterized by catecholamine-secreting activity. Pheochromocytomas account for 1.7% of pediatric hypertension cases. Surgical resection, the definitive pheochromocytoma treatment, carries risks of hemodynamic instability and cardiovascular complications. Nevertheless, mortality rates decreased significantly in the latter half of the 20th century due to effective perioperative blood pressure (BP) management. The literature on BP management tailored to pediatric pheochromocytoma is limited, while the sustained hypertension rate in this population is high (up to 90%) and related to a high risk of intraoperative complications. In this narrative review, we provide up-to-date recommendations regarding BP management to minimize perioperative comorbidities in children with pheochromocytoma.
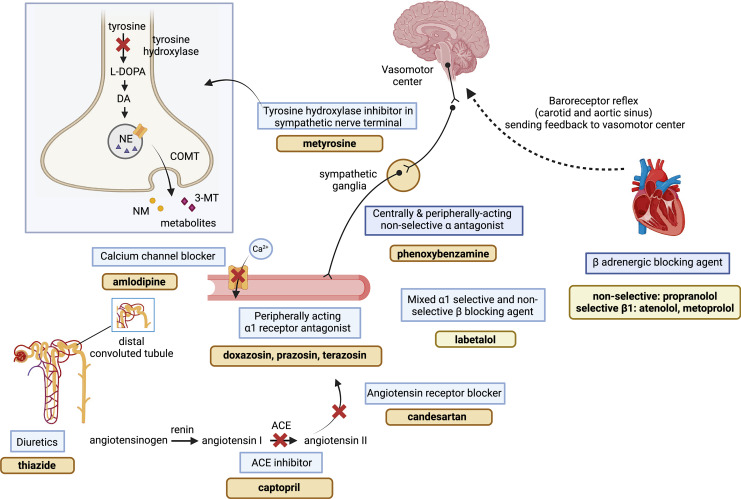
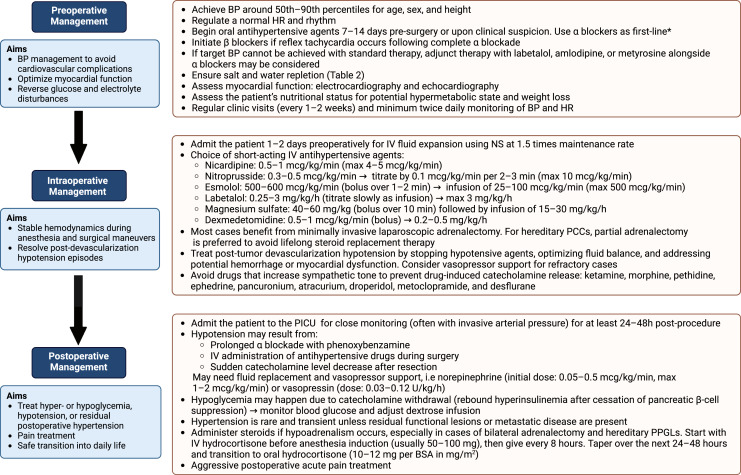
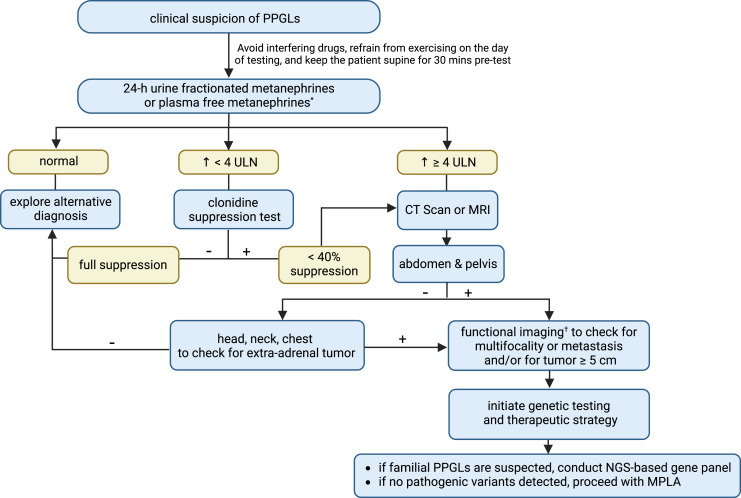
Summary: Antihypertensive agents, primarily alpha (α)-blockers, should be promptly administered for suspected pheochromocytoma. Beta (β)-blockers may be introduced thereafter to counteract reflex tachycardia. The patient must be salt- and water-replete preoperation. Intraoperatively, stable hemodynamics should be ensured during anesthesia and surgery, and short-acting intravenous medications and resuscitation fluid should be supplied. Postoperatively, patients should be admitted to the pediatric intensive care unit for close monitoring for at least 24-48 h. Genetic testing is recommended for all pheochromocytoma patients. Identifying underlying mutations, like in succinate dehydrogenase subunit B, which is linked to a higher risk of multifocality and metastasis, is imperative for tailoring treatment strategies and prognostication.
Key messages: Achieving optimal outcomes in pediatric pheochromocytoma relies on preoperative BP optimization with appropriate antihypertensive agents, intraoperative hemodynamic stability, and postoperative routine long-term follow-up to monitor for complications, recurrence, and metastasis. Future research should prioritize well-designed prospective multicenter studies with adequate sample sizes and, where feasible, randomized controlled trials with standardized protocols and appropriate endpoints. These studies should focus on the efficacy and safety of preoperative nonselective versus selective α-blockers, whether as monotherapy or combined with other medications (e.g., calcium channel blockers and/or β-blockers), or treatment without preoperative anti-hypertensives.
期刊介绍:
This journal comprises both clinical and basic studies at the interface of nephrology, hypertension and cardiovascular research. The topics to be covered include the structural organization and biochemistry of the normal and diseased kidney, the molecular biology of transporters, the physiology and pathophysiology of glomerular filtration and tubular transport, endothelial and vascular smooth muscle cell function and blood pressure control, as well as water, electrolyte and mineral metabolism. Also discussed are the (patho)physiology and (patho) biochemistry of renal hormones, the molecular biology, genetics and clinical course of renal disease and hypertension, the renal elimination, action and clinical use of drugs, as well as dialysis and transplantation. Featuring peer-reviewed original papers, editorials translating basic science into patient-oriented research and disease, in depth reviews, and regular special topic sections, ''Kidney & Blood Pressure Research'' is an important source of information for researchers in nephrology and cardiovascular medicine.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
