Information Mode-Dependent Success Rates of Obtaining German Medical Informatics Initiative-Compliant Broad Consent in the Emergency Department: Single-Center Prospective Observational Study.
Felix Patricius Hans, Jan Kleinekort, Melanie Boerries, Alexandra Nieters, Gerhard Kindle, Micha Rautenberg, Laura Bühler, Gerda Weiser, Michael Clemens Röttger, Carolin Neufischer, Matthias Kühn, Julius Wehrle, Anna Slagman, Antje Fischer-Rosinsky, Larissa Eienbröker, Frank Hanses, Gisbert Wilhelm Teepe, Hans-Jörg Busch, Leo Benning
{"title":"Information Mode-Dependent Success Rates of Obtaining German Medical Informatics Initiative-Compliant Broad Consent in the Emergency Department: Single-Center Prospective Observational Study.","authors":"Felix Patricius Hans, Jan Kleinekort, Melanie Boerries, Alexandra Nieters, Gerhard Kindle, Micha Rautenberg, Laura Bühler, Gerda Weiser, Michael Clemens Röttger, Carolin Neufischer, Matthias Kühn, Julius Wehrle, Anna Slagman, Antje Fischer-Rosinsky, Larissa Eienbröker, Frank Hanses, Gisbert Wilhelm Teepe, Hans-Jörg Busch, Leo Benning","doi":"10.2196/65646","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The broad consent (BC) developed by the German Medical Informatics Initiative is a pivotal national strategy for obtaining patient consent to use routinely collected data from electronic health records, insurance companies, contact information, and biomaterials for research. Emergency departments (EDs) are ideal for enrolling diverse patient populations in research activities. Despite regulatory and ethical challenges, obtaining BC from patients in ED with varying demographic, socioeconomic, and disease characteristics presents a promising opportunity to expand the availability of ED data.</p><p><strong>Objective: </strong>This study aimed to evaluate the success rate of obtaining BC through different consenting approaches in a tertiary ED and to explore factors influencing consent and dropout rates.</p><p><strong>Methods: </strong>A single-center prospective observational study was conducted in a German tertiary ED from September to December 2022. Every 30th patient was screened for eligibility. Eligible patients were informed via one of three modalities: (1) directly in the ED, (2) during their inpatient stay on the ward, or (3) via telephone after discharge. The primary outcome was the success rate of obtaining BC within 30 days of ED presentation. Secondary outcomes included analyzing potential influences on the success and dropout rates based on patient characteristics, information mode, and the interaction time required for patients to make an informed decision.</p><p><strong>Results: </strong>Of 11,842 ED visits, 419 patients were screened for BC eligibility, with 151 meeting the inclusion criteria. Of these, 68 (45%) consented to at least 1 BC module, while 24 (15.9%) refused participation. The dropout rate was 39.1% (n=59) and was highest in the telephone-based group (57/109, 52.3%) and lowest in the ED group (1/14, 7.1%). Patients informed face-to-face during their inpatient stay following the ED treatment had the highest consent rate (23/27, 85.2%), while those approached in the ED or by telephone had consent rates of 69.2% (9/13 and 36/52). Logistic regression analysis indicated that longer interaction time significantly improved consent rates (P=.03), while female sex was associated with higher dropout rates (P=.02). Age, triage category, billing details (inpatient treatment), or diagnosis did not significantly influence the primary outcome (all P>.05).</p><p><strong>Conclusions: </strong>Obtaining BC in an ED environment is feasible, enabling representative inclusion of ED populations. However, discharge from the ED and female sex negatively affected consent rates to the BC. Face-to-face interaction proved most effective, particularly for inpatients, while telephone-based approaches resulted in higher dropout rates despite comparable consent rates to direct consenting in the ED. The findings underscore the importance of tailored consent strategies and maintaining consenting staff in EDs and on the wards to enhance BC information delivery and consent processes for eligible patients.</p><p><strong>Trial registration: </strong>German Clinical Trials Register DRKS00028753; https://drks.de/search/de/trial/DRKS00028753.</p>","PeriodicalId":56334,"journal":{"name":"JMIR Medical Informatics","volume":" ","pages":"e65646"},"PeriodicalIF":3.8000,"publicationDate":"2024-12-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11688594/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Medical Informatics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2196/65646","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICAL INFORMATICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The broad consent (BC) developed by the German Medical Informatics Initiative is a pivotal national strategy for obtaining patient consent to use routinely collected data from electronic health records, insurance companies, contact information, and biomaterials for research. Emergency departments (EDs) are ideal for enrolling diverse patient populations in research activities. Despite regulatory and ethical challenges, obtaining BC from patients in ED with varying demographic, socioeconomic, and disease characteristics presents a promising opportunity to expand the availability of ED data.
Objective: This study aimed to evaluate the success rate of obtaining BC through different consenting approaches in a tertiary ED and to explore factors influencing consent and dropout rates.
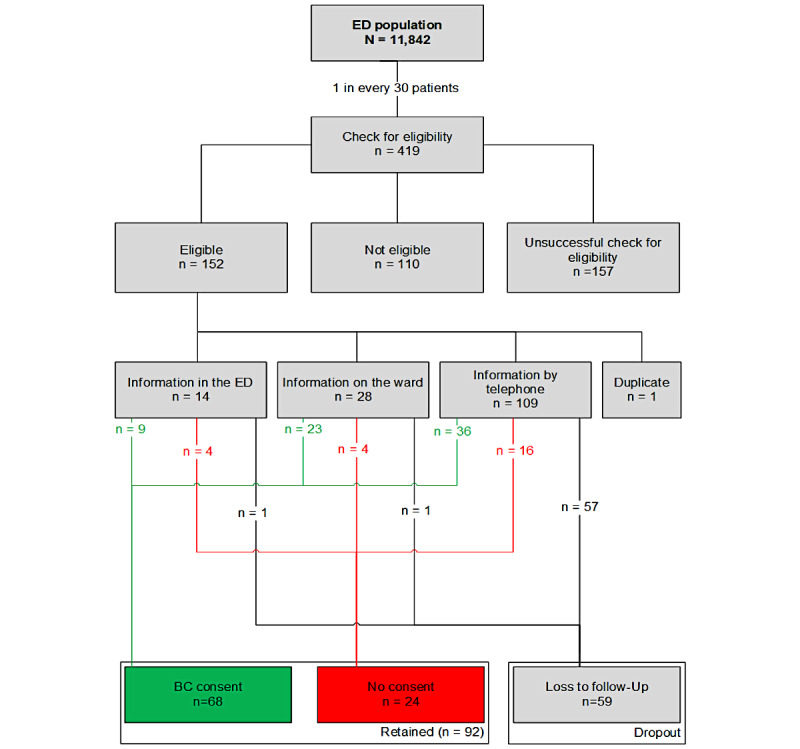
Methods: A single-center prospective observational study was conducted in a German tertiary ED from September to December 2022. Every 30th patient was screened for eligibility. Eligible patients were informed via one of three modalities: (1) directly in the ED, (2) during their inpatient stay on the ward, or (3) via telephone after discharge. The primary outcome was the success rate of obtaining BC within 30 days of ED presentation. Secondary outcomes included analyzing potential influences on the success and dropout rates based on patient characteristics, information mode, and the interaction time required for patients to make an informed decision.
Results: Of 11,842 ED visits, 419 patients were screened for BC eligibility, with 151 meeting the inclusion criteria. Of these, 68 (45%) consented to at least 1 BC module, while 24 (15.9%) refused participation. The dropout rate was 39.1% (n=59) and was highest in the telephone-based group (57/109, 52.3%) and lowest in the ED group (1/14, 7.1%). Patients informed face-to-face during their inpatient stay following the ED treatment had the highest consent rate (23/27, 85.2%), while those approached in the ED or by telephone had consent rates of 69.2% (9/13 and 36/52). Logistic regression analysis indicated that longer interaction time significantly improved consent rates (P=.03), while female sex was associated with higher dropout rates (P=.02). Age, triage category, billing details (inpatient treatment), or diagnosis did not significantly influence the primary outcome (all P>.05).
Conclusions: Obtaining BC in an ED environment is feasible, enabling representative inclusion of ED populations. However, discharge from the ED and female sex negatively affected consent rates to the BC. Face-to-face interaction proved most effective, particularly for inpatients, while telephone-based approaches resulted in higher dropout rates despite comparable consent rates to direct consenting in the ED. The findings underscore the importance of tailored consent strategies and maintaining consenting staff in EDs and on the wards to enhance BC information delivery and consent processes for eligible patients.
Trial registration: German Clinical Trials Register DRKS00028753; https://drks.de/search/de/trial/DRKS00028753.
期刊介绍:
JMIR Medical Informatics (JMI, ISSN 2291-9694) is a top-rated, tier A journal which focuses on clinical informatics, big data in health and health care, decision support for health professionals, electronic health records, ehealth infrastructures and implementation. It has a focus on applied, translational research, with a broad readership including clinicians, CIOs, engineers, industry and health informatics professionals.
Published by JMIR Publications, publisher of the Journal of Medical Internet Research (JMIR), the leading eHealth/mHealth journal (Impact Factor 2016: 5.175), JMIR Med Inform has a slightly different scope (emphasizing more on applications for clinicians and health professionals rather than consumers/citizens, which is the focus of JMIR), publishes even faster, and also allows papers which are more technical or more formative than what would be published in the Journal of Medical Internet Research.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
