{"title":"Baseline systolic blood pressure and efficacy of dual antiplatelet in acute ischaemic stroke.","authors":"Yu Cui, Yue Wang, Hui-Sheng Chen","doi":"10.1136/svn-2024-003615","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Systolic blood pressure (SBP) affects the risk of early neurological deterioration (END). This subgroup analysis of Antiplatelet Therapy in Acute Mild to Moderate Ischemic Stroke (ATAMIS) trial aimed to explore whether SBP at admission affected the efficacy of different antiplatelet therapies in preventing END.</p><p><strong>Methods: </strong>Based on the modified intention-to-treat analysis set of the ATAMIS trial, patients were divided into two subgroups according to whether SBP at admission was equal to or higher than 140 mm Hg, which were further subdivided into clopidogrel plus aspirin and aspirin alone treatments according to the randomised assignment. We conducted multivariable regression analyses to detect relationship between SBP at admission and END, as well as efficacy of different antiplatelet therapies in each SBP subgroup. Primary endpoint was END defined as ≥2-point increase in 7-day National Institutes of Health Stroke Scale score. Safety endpoints included intracranial haemorrhage and bleeding events during the trial.</p><p><strong>Results: </strong>This study included 2915 patients. Risk of END raised by 16% as SBP at admission increased by every 10 mm Hg (p<0.001). Clopidogrel plus aspirin resulted in significantly lower risk of END than aspirin alone in patients with SBP≥140 mm Hg (5.5% vs 7.9%; adjusted risk difference (RD) and 95% CI -2.5% (-4.1% to -1.0%)), but not in those with SBP<140 mm Hg (3.4% vs 4.2%; adjusted RD and 95% CI -0.8% (-3.2% to 1.7%)). Efficacy of different antiplatelet therapies and SBP did not show significant interaction (p=0.50). Safety endpoints were similar between treatments in SBP subgroups.</p><p><strong>Conclusion: </strong>The risk of END increases with elevated SBP at admission among patients with acute mild-to-moderate ischaemic stroke who are not suitable for reperfusion treatments. Fewer END occurred following clopidogrel plus aspirin compared with aspirin alone across different SBP levels. The finding should be interpreted cautiously.</p>","PeriodicalId":48733,"journal":{"name":"Journal of Investigative Medicine","volume":" ","pages":"481-490"},"PeriodicalIF":4.9000,"publicationDate":"2025-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12415644/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Investigative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/svn-2024-003615","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Systolic blood pressure (SBP) affects the risk of early neurological deterioration (END). This subgroup analysis of Antiplatelet Therapy in Acute Mild to Moderate Ischemic Stroke (ATAMIS) trial aimed to explore whether SBP at admission affected the efficacy of different antiplatelet therapies in preventing END.
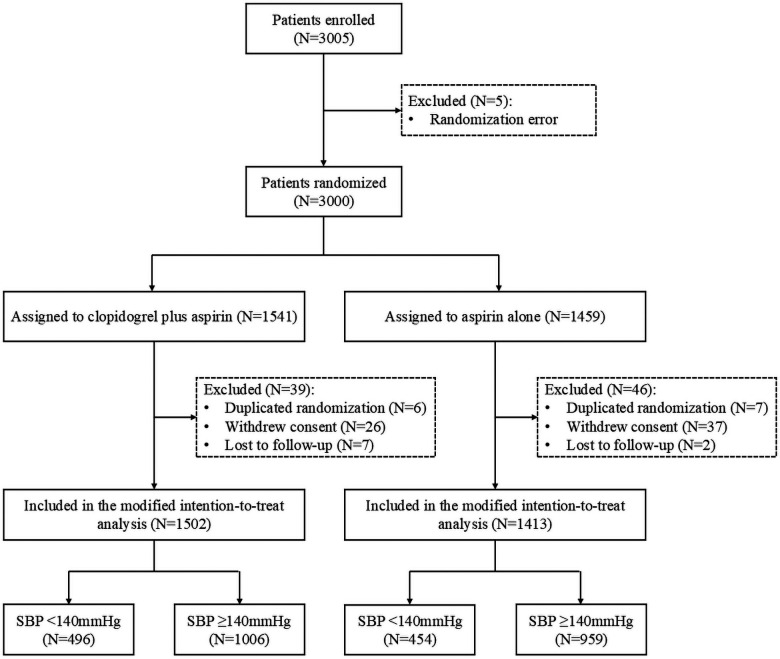
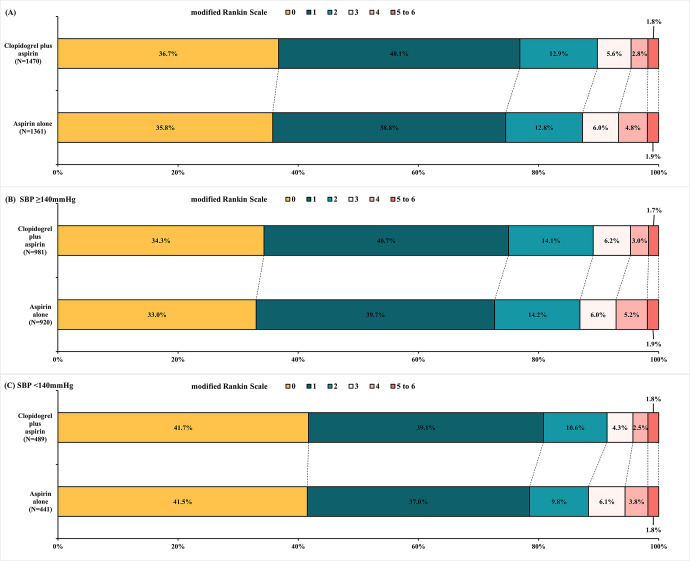
Methods: Based on the modified intention-to-treat analysis set of the ATAMIS trial, patients were divided into two subgroups according to whether SBP at admission was equal to or higher than 140 mm Hg, which were further subdivided into clopidogrel plus aspirin and aspirin alone treatments according to the randomised assignment. We conducted multivariable regression analyses to detect relationship between SBP at admission and END, as well as efficacy of different antiplatelet therapies in each SBP subgroup. Primary endpoint was END defined as ≥2-point increase in 7-day National Institutes of Health Stroke Scale score. Safety endpoints included intracranial haemorrhage and bleeding events during the trial.
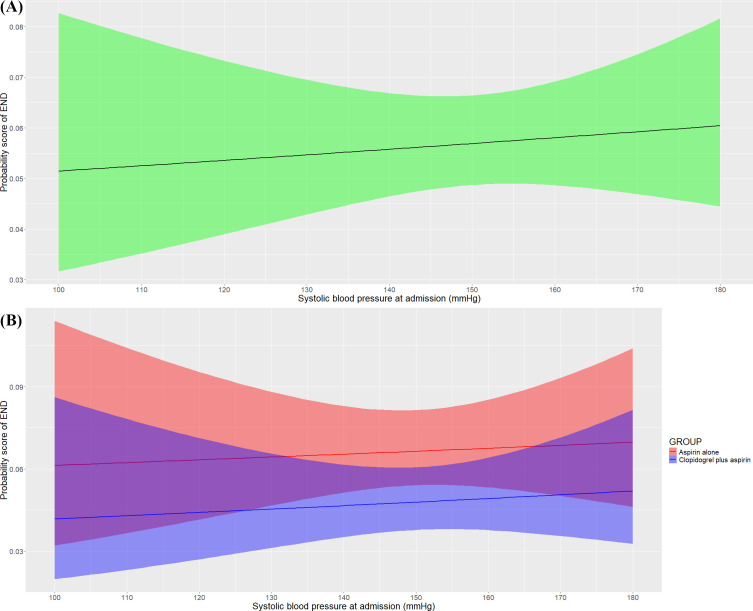
Results: This study included 2915 patients. Risk of END raised by 16% as SBP at admission increased by every 10 mm Hg (p<0.001). Clopidogrel plus aspirin resulted in significantly lower risk of END than aspirin alone in patients with SBP≥140 mm Hg (5.5% vs 7.9%; adjusted risk difference (RD) and 95% CI -2.5% (-4.1% to -1.0%)), but not in those with SBP<140 mm Hg (3.4% vs 4.2%; adjusted RD and 95% CI -0.8% (-3.2% to 1.7%)). Efficacy of different antiplatelet therapies and SBP did not show significant interaction (p=0.50). Safety endpoints were similar between treatments in SBP subgroups.
Conclusion: The risk of END increases with elevated SBP at admission among patients with acute mild-to-moderate ischaemic stroke who are not suitable for reperfusion treatments. Fewer END occurred following clopidogrel plus aspirin compared with aspirin alone across different SBP levels. The finding should be interpreted cautiously.
目的:收缩压(SBP)影响早期神经功能恶化(END)的风险。本亚组分析急性轻中度缺血性卒中抗血小板治疗(ATAMIS)试验旨在探讨入院时收缩压是否影响不同抗血小板治疗预防END的疗效。方法:以ATAMIS试验改良意向治疗分析集为基础,根据入院时收缩压是否等于或高于140 mm Hg将患者分为2个亚组,再根据随机分配进一步分为氯吡格雷加阿司匹林和阿司匹林单用治疗。我们进行了多变量回归分析,以检测入院时收缩压与终末期的关系,以及不同抗血小板治疗在收缩压亚组中的疗效。主要终点END定义为7天美国国立卫生研究院卒中量表评分增加≥2分。安全性终点包括颅内出血和试验期间的出血事件。结果:本研究纳入2915例患者。结论:不适合再灌注治疗的急性轻中度缺血性脑卒中患者入院时收缩压升高,END风险增加16%。在不同收缩压水平下,氯吡格雷加阿司匹林比单独服用阿司匹林更少发生END。这一发现应该谨慎解读。
期刊介绍:
Journal of Investigative Medicine (JIM) is the official publication of the American Federation for Medical Research. The journal is peer-reviewed and publishes high-quality original articles and reviews in the areas of basic, clinical, and translational medical research.
JIM publishes on all topics and specialty areas that are critical to the conduct of the entire spectrum of biomedical research: from the translation of clinical observations at the bedside, to basic and animal research to clinical research and the implementation of innovative medical care.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
