Esra Kochan Kizilkilic, Nursena Erener, Mustafa Meric, Nurten Uzun Adatepe, Aysegul Gunduz
{"title":"Risk of Spreading in Adult-onset Dystonia.","authors":"Esra Kochan Kizilkilic, Nursena Erener, Mustafa Meric, Nurten Uzun Adatepe, Aysegul Gunduz","doi":"10.5334/tohm.952","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adult-onset dystonia can also spread to other parts of the body, although it is not as common as childhood-onset dystonia.</p><p><strong>Objective: </strong>Our study aimed to examine the clinical factors determining spreading patterns in all adult-onset dystonia types.</p><p><strong>Methods: </strong>We retrospectively analyzed the medical records of patients with a diagnosis of isolated dystonia followed longitudinally at our center. We included patients reporting symptom onset after 18 years. We then compared the clinical factors between groups with and without spreading.</p><p><strong>Results: </strong>Among 434 patients (396 focal, 29 segmental, and nine generalized onset dystonia. mean follow-up of 8.6 ± 7.8 years), 48 (11.1%) experienced spread of dystonia, with 37 progressing from focal to segmental, two from focal to generalized, two from segmental to generalized, and seven from focal to segmental to generalized dystonia. Blepharospasm was the most common focal dystonia noted to spread, followed by oromandibular dystonia, cervical dystonia, laryngeal dystonia, and upper extremity dystonia, in decreasing order. A spreading pattern was observed in approximately one in 10 dystonia patients, and the spreading was more frequent in the segmental dystonia group. While there was no difference between the spreading groups regarding sensory tricks, tremor, and gender, family history was more common in the non-spreading group (p = 0.023). Older age at onset was independently associated with increased odds of spreading (hazards ratio: 1.054, p < 0.001, B = 0.053).</p><p><strong>Conclusion: </strong>Although risk factors for spread are variable, the underlying mechanisms are not fully known. Genetic factors may be possibly related to the spread, and future studies are needed on this subject.</p>","PeriodicalId":23317,"journal":{"name":"Tremor and Other Hyperkinetic Movements","volume":"14 ","pages":"59"},"PeriodicalIF":2.1000,"publicationDate":"2024-12-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11623075/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tremor and Other Hyperkinetic Movements","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5334/tohm.952","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Adult-onset dystonia can also spread to other parts of the body, although it is not as common as childhood-onset dystonia.
Objective: Our study aimed to examine the clinical factors determining spreading patterns in all adult-onset dystonia types.
Methods: We retrospectively analyzed the medical records of patients with a diagnosis of isolated dystonia followed longitudinally at our center. We included patients reporting symptom onset after 18 years. We then compared the clinical factors between groups with and without spreading.
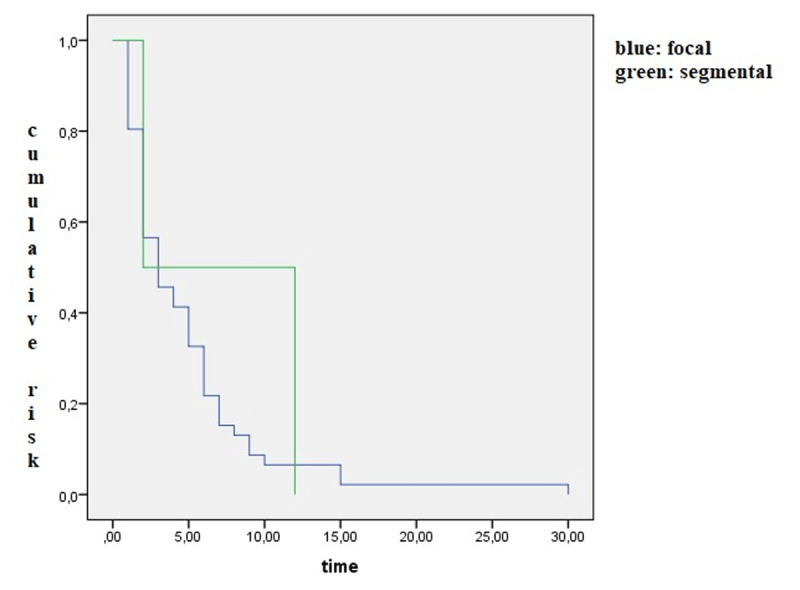
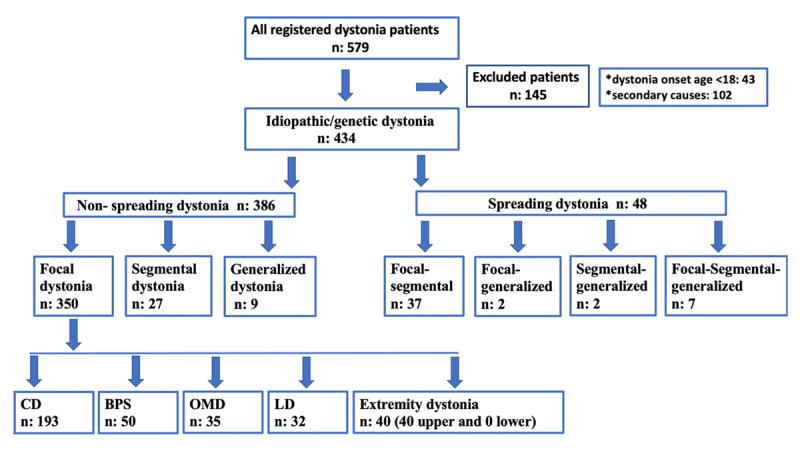
Results: Among 434 patients (396 focal, 29 segmental, and nine generalized onset dystonia. mean follow-up of 8.6 ± 7.8 years), 48 (11.1%) experienced spread of dystonia, with 37 progressing from focal to segmental, two from focal to generalized, two from segmental to generalized, and seven from focal to segmental to generalized dystonia. Blepharospasm was the most common focal dystonia noted to spread, followed by oromandibular dystonia, cervical dystonia, laryngeal dystonia, and upper extremity dystonia, in decreasing order. A spreading pattern was observed in approximately one in 10 dystonia patients, and the spreading was more frequent in the segmental dystonia group. While there was no difference between the spreading groups regarding sensory tricks, tremor, and gender, family history was more common in the non-spreading group (p = 0.023). Older age at onset was independently associated with increased odds of spreading (hazards ratio: 1.054, p < 0.001, B = 0.053).
Conclusion: Although risk factors for spread are variable, the underlying mechanisms are not fully known. Genetic factors may be possibly related to the spread, and future studies are needed on this subject.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
