Nicola K Wills, Jared Tavares, Qonita Said-Hartley, Sean Wasserman
{"title":"Radiological predictors of PCP in HIV-positive adults in South Africa: A matched case-control study.","authors":"Nicola K Wills, Jared Tavares, Qonita Said-Hartley, Sean Wasserman","doi":"10.4102/sajhivmed.v25i1.1636","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Definition of chest X-ray (CXR) features associated with laboratory-confirmed pneumocystis pneumonia (PCP) among HIV-positive adults is needed to improve diagnosis in high-burden settings.</p><p><strong>Objectives: </strong>Our primary objective was to identify CXR features associated with confirmed PCP diagnosis and severe PCP (defined by hypoxia, intensive care unit referral/admission, and/or in-hospital death). We also explored the performance of logistic regression models, incorporating selected clinical and CXR predictors, for PCP diagnosis and severe PCP.</p><p><strong>Method: </strong>We conducted a case-control study involving HIV-positive adults with laboratory-confirmed PCP and a matched cohort with non-PCP respiratory presentations at regional hospitals in Cape Town, South Africa (2012-2020).</p><p><strong>Results: </strong>Records from 104 adults (52 PCP cases and 52 non-PCP controls) were included. Diffuse versus patchy ground-glass opacification was associated with increased odds of PCP diagnosis (adjusted odds ratio [aOR]: 6.2, 95% confidence interval [CI]: 1.6-28.9, <i>P</i> = 0.01) and severe PCP (aOR: 4.5, 95% CI: 1.6-14.4, <i>P</i> = 0.008). Consolidation was associated with severe PCP (aOR: 3.3, 95% CI: 1.2-11.0, <i>P</i> = 0.03) as was increasing ground-glass zone involvement (aOR: 2.1 for each one-unit increase in involved zone; 95% CI: 1.4-3.2, <i>P</i> = 0.0004). Models incorporating hypoxia (hypoxia model) or tachypnoea (respiratory rate model) with diffuse ground-glass opacities, absence of pleural effusion or reticular/reticulonodular changes on CXR performed well in predicting PCP (area under the receiver operating characteristic curve 0.828 [hypoxia model] and 0.857 [respiratory rate model]).</p><p><strong>Conclusion: </strong>CXR evaluation alongside bedside clinical information offers good accuracy for discriminating definite PCP from other HIV-associated respiratory diseases.</p>","PeriodicalId":94212,"journal":{"name":"Southern African journal of HIV medicine","volume":"25 1","pages":"1636"},"PeriodicalIF":2.3000,"publicationDate":"2024-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11622136/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Southern African journal of HIV medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4102/sajhivmed.v25i1.1636","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Definition of chest X-ray (CXR) features associated with laboratory-confirmed pneumocystis pneumonia (PCP) among HIV-positive adults is needed to improve diagnosis in high-burden settings.
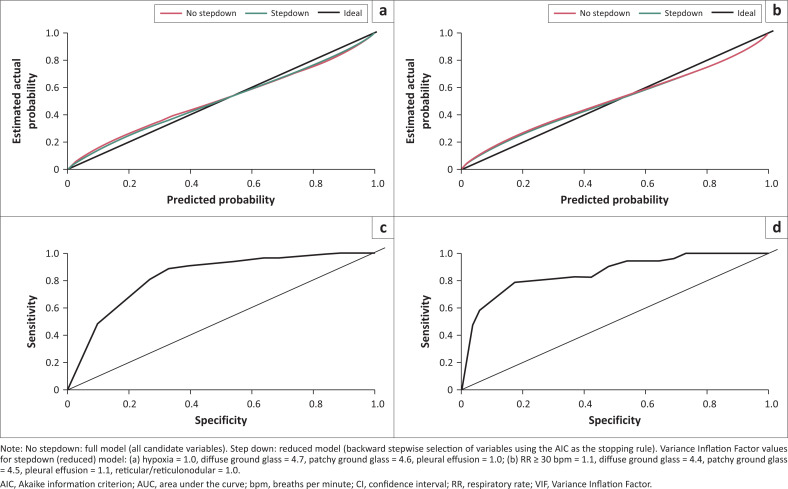
Objectives: Our primary objective was to identify CXR features associated with confirmed PCP diagnosis and severe PCP (defined by hypoxia, intensive care unit referral/admission, and/or in-hospital death). We also explored the performance of logistic regression models, incorporating selected clinical and CXR predictors, for PCP diagnosis and severe PCP.
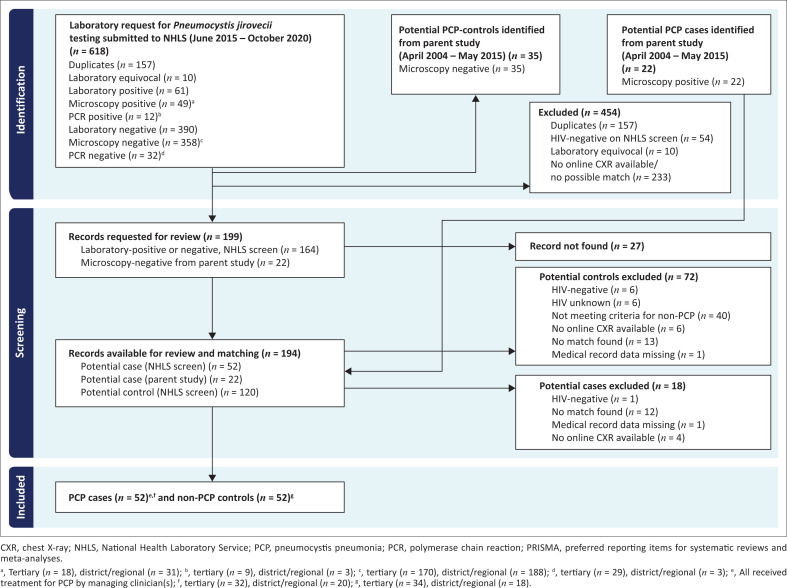
Method: We conducted a case-control study involving HIV-positive adults with laboratory-confirmed PCP and a matched cohort with non-PCP respiratory presentations at regional hospitals in Cape Town, South Africa (2012-2020).
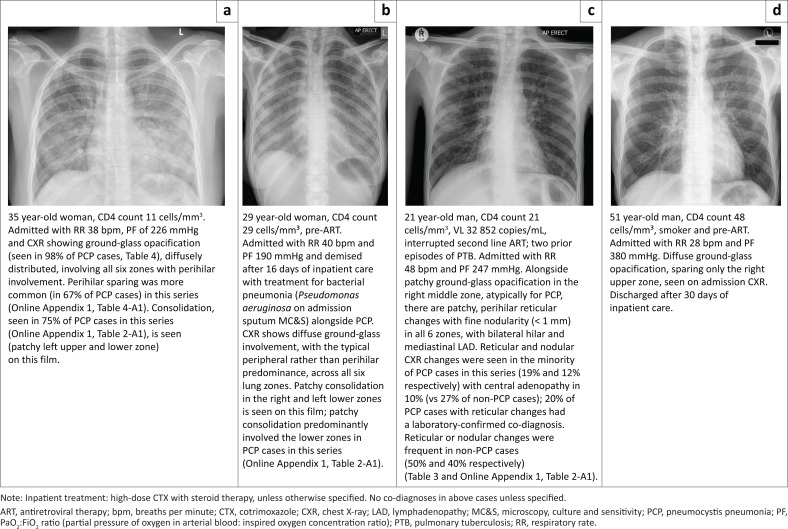
Results: Records from 104 adults (52 PCP cases and 52 non-PCP controls) were included. Diffuse versus patchy ground-glass opacification was associated with increased odds of PCP diagnosis (adjusted odds ratio [aOR]: 6.2, 95% confidence interval [CI]: 1.6-28.9, P = 0.01) and severe PCP (aOR: 4.5, 95% CI: 1.6-14.4, P = 0.008). Consolidation was associated with severe PCP (aOR: 3.3, 95% CI: 1.2-11.0, P = 0.03) as was increasing ground-glass zone involvement (aOR: 2.1 for each one-unit increase in involved zone; 95% CI: 1.4-3.2, P = 0.0004). Models incorporating hypoxia (hypoxia model) or tachypnoea (respiratory rate model) with diffuse ground-glass opacities, absence of pleural effusion or reticular/reticulonodular changes on CXR performed well in predicting PCP (area under the receiver operating characteristic curve 0.828 [hypoxia model] and 0.857 [respiratory rate model]).
Conclusion: CXR evaluation alongside bedside clinical information offers good accuracy for discriminating definite PCP from other HIV-associated respiratory diseases.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
