{"title":"Prolonged weaning from mechanical ventilation: who, what, when and how?","authors":"Neeraj M Shah, Nicholas Hart, Georgios Kaltsakas","doi":"10.1183/20734735.0122-2024","DOIUrl":null,"url":null,"abstract":"<p><p>Weaning from invasive mechanical ventilation is an important part of the management of respiratory failure patients. Patients can be classified into those who wean on the first attempt (simple weaning), those who require up to three attempts (difficult weaning) and those who require more than three attempts (prolonged weaning). The process of weaning includes adequately treating the underlying cause of respiratory failure, assessing the readiness to wean, evaluating the response to a reduction in ventilatory support, and eventually liberation from mechanical ventilation and extubation or decannulation. Post-extubation respiratory failure is a contributor to poorer outcomes. Identifying and addressing modifiable risk factors for post-extubation respiratory failure is important; noninvasive ventilation and high-flow nasal cannulae may be useful bridging aids after extubation. Factors to consider in the pathophysiology of prolonged mechanical ventilation include increased respiratory muscle load, reduced respiratory muscle capacity and reduced respiratory drive. Management of these patients involves a multidisciplinary team, to first identify the cause of failed weaning attempts, and subsequently optimise the patient's physiology to improve the likelihood of being successfully weaned from invasive mechanical ventilation.</p>","PeriodicalId":9292,"journal":{"name":"Breathe","volume":"20 3","pages":"240122"},"PeriodicalIF":3.4000,"publicationDate":"2024-12-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11629167/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Breathe","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1183/20734735.0122-2024","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
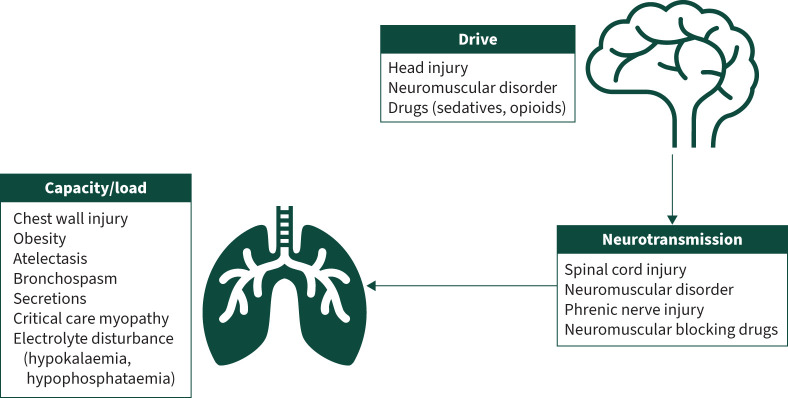
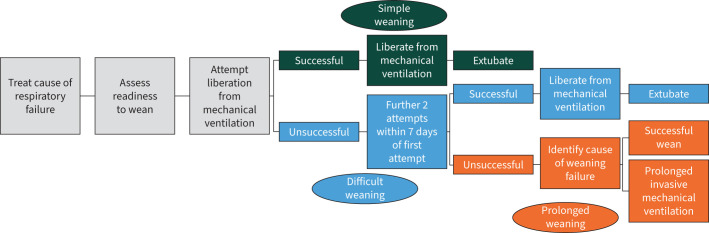
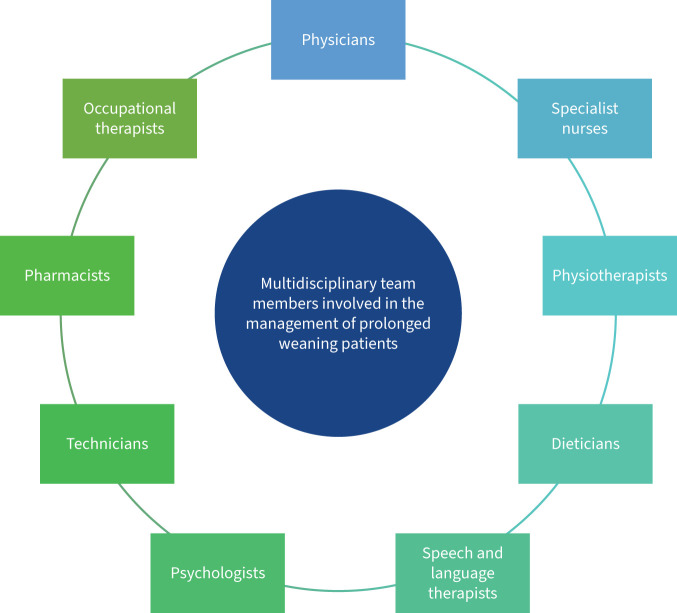
Weaning from invasive mechanical ventilation is an important part of the management of respiratory failure patients. Patients can be classified into those who wean on the first attempt (simple weaning), those who require up to three attempts (difficult weaning) and those who require more than three attempts (prolonged weaning). The process of weaning includes adequately treating the underlying cause of respiratory failure, assessing the readiness to wean, evaluating the response to a reduction in ventilatory support, and eventually liberation from mechanical ventilation and extubation or decannulation. Post-extubation respiratory failure is a contributor to poorer outcomes. Identifying and addressing modifiable risk factors for post-extubation respiratory failure is important; noninvasive ventilation and high-flow nasal cannulae may be useful bridging aids after extubation. Factors to consider in the pathophysiology of prolonged mechanical ventilation include increased respiratory muscle load, reduced respiratory muscle capacity and reduced respiratory drive. Management of these patients involves a multidisciplinary team, to first identify the cause of failed weaning attempts, and subsequently optimise the patient's physiology to improve the likelihood of being successfully weaned from invasive mechanical ventilation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
