Primary Results of Our Protocol for Standardization of Perioperative Antiplatelet Agent Management on the Incidence of Epidural Hematoma and Thrombotic Complications in Posterior Cervical Surgery: A Prospective Cohort Study.
{"title":"Primary Results of Our Protocol for Standardization of Perioperative Antiplatelet Agent Management on the Incidence of Epidural Hematoma and Thrombotic Complications in Posterior Cervical Surgery: A Prospective Cohort Study.","authors":"Gentaro Kumagai, Kanichiro Wada, Toru Asari, Yoshiro Nitobe, Kotaro Aburakawa, Yasuyuki Ishibashi","doi":"10.22603/ssrr.2024-0017","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>This study aimed to standardize perioperative interruption of antiplatelet agents in patients undergoing cervical spinal surgery and investigate the incidence of epidural hematoma and thrombotic complications.</p><p><strong>Methods: </strong>A total of 153 patients, consisting of 85 men and 68 women, were included in this study. Their mean age was 65.5 years. They were divided into two groups: Groups A and B. Group A (139 patients) did not receive preoperative antiplatelet agents, and Group B (14 patients) resumed antiplatelet agents from 7 or 14 days presurgery to 3 days postsurgery. Our analysis encompassed demographic data before surgery, postoperative magnetic resonance image-based assessment of radiological epidural hematoma (EH), and complications such as symptomatic hematoma, blood transfusion, stroke, and venous thromboembolism after surgery.</p><p><strong>Results: </strong>The frequency of medical conditions, such as hypertension, diabetes, and hyperlipidemia, was significantly higher in Group B than in Group A. The CHADS2 scores, which serve as a clinical prediction rule for estimating stroke risk, were significantly higher in Group B than in Group A. In contrast, the intraoperative blood loss was significantly lower in Group B than in Group A. There was no significant difference in radiologically severe EH, hemorrhage, and thrombotic complications between the two groups. Interestingly, none of the patients in Group B had hemorrhagic and thrombotic complications.</p><p><strong>Conclusions: </strong>Our standardized perioperative management of antiplatelet agents did not affect the incidence of radiological EH, hemorrhage, and thrombotic complications in patients undergoing cervical spinal surgery.</p>","PeriodicalId":22253,"journal":{"name":"Spine Surgery and Related Research","volume":"8 6","pages":"568-574"},"PeriodicalIF":1.2000,"publicationDate":"2024-05-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11625718/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22603/ssrr.2024-0017","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/27 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: This study aimed to standardize perioperative interruption of antiplatelet agents in patients undergoing cervical spinal surgery and investigate the incidence of epidural hematoma and thrombotic complications.
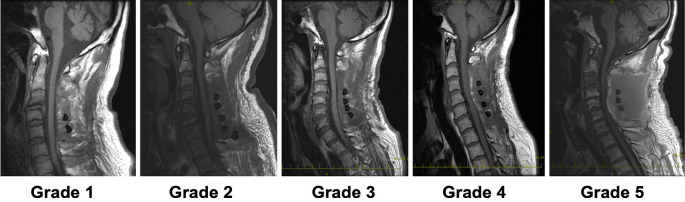
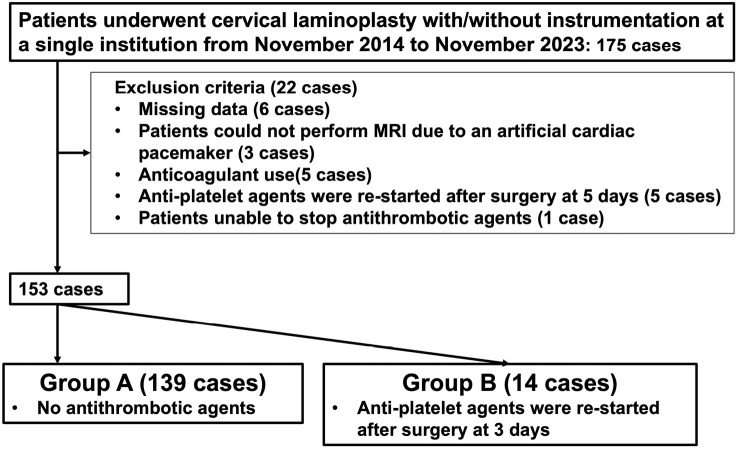
Methods: A total of 153 patients, consisting of 85 men and 68 women, were included in this study. Their mean age was 65.5 years. They were divided into two groups: Groups A and B. Group A (139 patients) did not receive preoperative antiplatelet agents, and Group B (14 patients) resumed antiplatelet agents from 7 or 14 days presurgery to 3 days postsurgery. Our analysis encompassed demographic data before surgery, postoperative magnetic resonance image-based assessment of radiological epidural hematoma (EH), and complications such as symptomatic hematoma, blood transfusion, stroke, and venous thromboembolism after surgery.
Results: The frequency of medical conditions, such as hypertension, diabetes, and hyperlipidemia, was significantly higher in Group B than in Group A. The CHADS2 scores, which serve as a clinical prediction rule for estimating stroke risk, were significantly higher in Group B than in Group A. In contrast, the intraoperative blood loss was significantly lower in Group B than in Group A. There was no significant difference in radiologically severe EH, hemorrhage, and thrombotic complications between the two groups. Interestingly, none of the patients in Group B had hemorrhagic and thrombotic complications.
Conclusions: Our standardized perioperative management of antiplatelet agents did not affect the incidence of radiological EH, hemorrhage, and thrombotic complications in patients undergoing cervical spinal surgery.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
