Paula M Kett, Grace A Guenther, Marieke S van Eijk, Davis G Patterson, Bianca K Frogner
{"title":"Low birthweight rate differences associated with distinct perinatal staffing mixes at federally funded health centers.","authors":"Paula M Kett, Grace A Guenther, Marieke S van Eijk, Davis G Patterson, Bianca K Frogner","doi":"10.1093/haschl/qxae113","DOIUrl":null,"url":null,"abstract":"<p><p>Health centers (sometimes referred to as \"federally qualified health centers\") can play an important role in addressing perinatal inequities. However, there is limited information on how different staffing models in health centers contribute to perinatal outcomes, including the availability of certified nurse midwives (CNMs). Using 2011-2021 Uniform Data System files, we examined 4 staffing models in 1385 health centers: those with no CNMs or obstetricians-gynecologists (OBs) (\"non-CNM/OB\"), CNM-only, OB-only, and both CNMs and OBs (\"CNM/OB\"). We predicted adjusted low birthweight (LBW) rates across these staffing types using a generalized linear model approach, adjusting for both time and center fixed effects as well as relevant patient, staffing, organizational, and community characteristics. We found that CNM-only health centers had the lowest LBW rates across all staffing models (7.6%) and non-CNM/OB centers had the highest (10.1%). Among Black births, LBW rates ranged from 10.1% (CNM-only) to 13.5% (non-CNM/OB). Findings indicate the importance of building and supporting the CNM workforce and ensuring adequate staffing at health centers, particularly as part of a comprehensive approach to addressing inequities in perinatal outcomes including addressing the scope of practice of CNMs, as more CNM-staff health centers were in areas with independent scope of practice.</p>","PeriodicalId":94025,"journal":{"name":"Health affairs scholar","volume":"2 12","pages":"qxae113"},"PeriodicalIF":2.7000,"publicationDate":"2024-12-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11630281/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health affairs scholar","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/haschl/qxae113","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
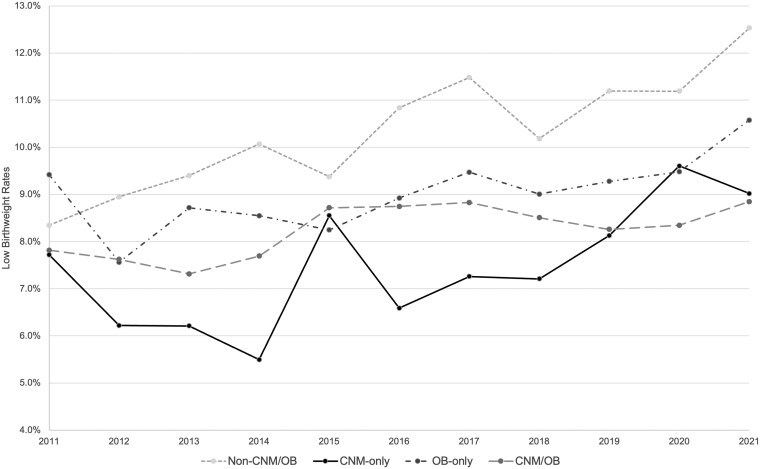
Health centers (sometimes referred to as "federally qualified health centers") can play an important role in addressing perinatal inequities. However, there is limited information on how different staffing models in health centers contribute to perinatal outcomes, including the availability of certified nurse midwives (CNMs). Using 2011-2021 Uniform Data System files, we examined 4 staffing models in 1385 health centers: those with no CNMs or obstetricians-gynecologists (OBs) ("non-CNM/OB"), CNM-only, OB-only, and both CNMs and OBs ("CNM/OB"). We predicted adjusted low birthweight (LBW) rates across these staffing types using a generalized linear model approach, adjusting for both time and center fixed effects as well as relevant patient, staffing, organizational, and community characteristics. We found that CNM-only health centers had the lowest LBW rates across all staffing models (7.6%) and non-CNM/OB centers had the highest (10.1%). Among Black births, LBW rates ranged from 10.1% (CNM-only) to 13.5% (non-CNM/OB). Findings indicate the importance of building and supporting the CNM workforce and ensuring adequate staffing at health centers, particularly as part of a comprehensive approach to addressing inequities in perinatal outcomes including addressing the scope of practice of CNMs, as more CNM-staff health centers were in areas with independent scope of practice.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
