Florence Joly, Fernando Bazan, Delphine Garbay, Yaelle Ouldbey, Philippe Follana, Élise Champeaux-Orange, Eric Legouffe, Pierre-Emmanuel Brachet, Dominique Spaeth, Pierre Combe, Anne-Claire Hardy-Bessard, Frédéric Selle, Julien Grenier, Coriolan Lebreton, Olfa Derbel, Elise Bonnet, Pierre Fournel, Yolanda Fernandez Diez, Valérie Delecroix, Sheik Emambux, Jérôme Alexandre, Thomas Grellety, Dominique Mille, Hubert Orfeuvre, Catherine Favier, Delphine Le Roux, Marie-Ange Mouret-Reynier, Stanislas Quesada, Jean-Emmanuel Kurtz
{"title":"Improving real-world evaluation of patient- and physician-reported tolerability: niraparib for recurrent ovarian cancer (NiQoLe).","authors":"Florence Joly, Fernando Bazan, Delphine Garbay, Yaelle Ouldbey, Philippe Follana, Élise Champeaux-Orange, Eric Legouffe, Pierre-Emmanuel Brachet, Dominique Spaeth, Pierre Combe, Anne-Claire Hardy-Bessard, Frédéric Selle, Julien Grenier, Coriolan Lebreton, Olfa Derbel, Elise Bonnet, Pierre Fournel, Yolanda Fernandez Diez, Valérie Delecroix, Sheik Emambux, Jérôme Alexandre, Thomas Grellety, Dominique Mille, Hubert Orfeuvre, Catherine Favier, Delphine Le Roux, Marie-Ange Mouret-Reynier, Stanislas Quesada, Jean-Emmanuel Kurtz","doi":"10.1093/jncics/pkae114","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Maintenance niraparib at an individualized starting dose (ISD) is established in platinum-sensitive recurrent ovarian cancer (PSROC). However, patients' perspectives on the burden of prolonged maintenance therapy have not been reported in prospective trials or routine practice.</p><p><strong>Methods: </strong>In the real-life multicenter NiQoLe study, patients with PSROC received ISD maintenance niraparib. The primary objective was to describe physician-reported adverse events (AEs) leading to treatment modification during the first 3 months. Secondary endpoints included patient-reported outcomes (symptomatic AEs using PRO-CTCAE, self-reported fatigue, and impact on daily activities/function using FACT-F) collected remotely weekly using a specifically designed electronic device.</p><p><strong>Results: </strong>Most (80%) of 139 treated patients (median age = 70 years) began niraparib at 200 mg/day. Median treatment duration was 5.7 (range = 0.2-21.4) months. During the first 3 months, 86 patients (62%) required treatment modification (median = 27 days to modification). Physician-reported grade ≥3 niraparib-related AEs occurred in 34 patients (24%); 68 patients (49%) had treatment modification for AEs, predominantly thrombocytopenia. The most frequent patient-reported AEs (PRO-CTCAE) were fatigue, insomnia, constipation, and dry mouth. Self-reported AEs were severe in 66% of patients. At baseline, 33% of patients reported severe fatigue (FACT-F), which generally persisted during niraparib. Physicians systematically underestimated major patient-reported symptoms.</p><p><strong>Conclusions: </strong>In routine practice, niraparib dose modification was often required during the first 3 months despite individualized dosing. Physicians underestimated the burden of fatigue and symptomatic AEs. Digital self-reporting of AEs is feasible, provides patient-centered information complementing physician-reported AEs, and allows fuller appreciation of toxicity in real-world studies.</p><p><strong>Clinical trial information: </strong>NCT03752216.</p>","PeriodicalId":14681,"journal":{"name":"JNCI Cancer Spectrum","volume":" ","pages":""},"PeriodicalIF":4.1000,"publicationDate":"2025-01-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11878563/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JNCI Cancer Spectrum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jncics/pkae114","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Maintenance niraparib at an individualized starting dose (ISD) is established in platinum-sensitive recurrent ovarian cancer (PSROC). However, patients' perspectives on the burden of prolonged maintenance therapy have not been reported in prospective trials or routine practice.
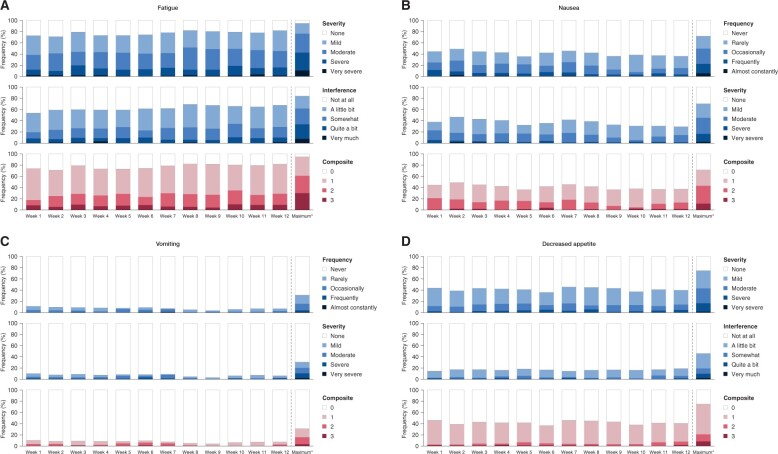
Methods: In the real-life multicenter NiQoLe study, patients with PSROC received ISD maintenance niraparib. The primary objective was to describe physician-reported adverse events (AEs) leading to treatment modification during the first 3 months. Secondary endpoints included patient-reported outcomes (symptomatic AEs using PRO-CTCAE, self-reported fatigue, and impact on daily activities/function using FACT-F) collected remotely weekly using a specifically designed electronic device.
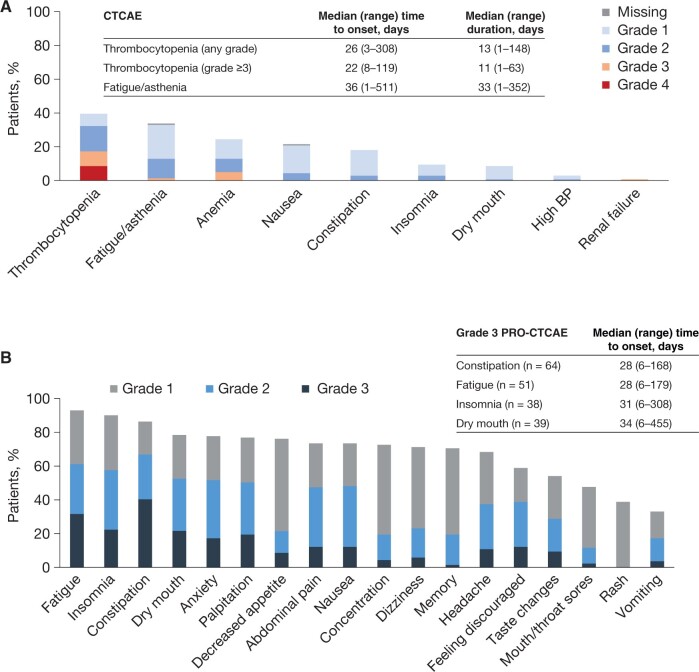
Results: Most (80%) of 139 treated patients (median age = 70 years) began niraparib at 200 mg/day. Median treatment duration was 5.7 (range = 0.2-21.4) months. During the first 3 months, 86 patients (62%) required treatment modification (median = 27 days to modification). Physician-reported grade ≥3 niraparib-related AEs occurred in 34 patients (24%); 68 patients (49%) had treatment modification for AEs, predominantly thrombocytopenia. The most frequent patient-reported AEs (PRO-CTCAE) were fatigue, insomnia, constipation, and dry mouth. Self-reported AEs were severe in 66% of patients. At baseline, 33% of patients reported severe fatigue (FACT-F), which generally persisted during niraparib. Physicians systematically underestimated major patient-reported symptoms.
Conclusions: In routine practice, niraparib dose modification was often required during the first 3 months despite individualized dosing. Physicians underestimated the burden of fatigue and symptomatic AEs. Digital self-reporting of AEs is feasible, provides patient-centered information complementing physician-reported AEs, and allows fuller appreciation of toxicity in real-world studies.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
