Giuliano Francesco Bonura, Paolo Biancheri, Joachim Rainer, Paola Soriani, Enrique Rodriguez de Santiago, Arianna Parrella, Alice Campioli, Emmanuele Guerra, Eugenia Gualdi, Alessandro Pignatti, Mauro Manno
{"title":"Spinal anesthesia for endoscopic submucosal dissection of large rectosigmoid lesions: Feasibility study.","authors":"Giuliano Francesco Bonura, Paolo Biancheri, Joachim Rainer, Paola Soriani, Enrique Rodriguez de Santiago, Arianna Parrella, Alice Campioli, Emmanuele Guerra, Eugenia Gualdi, Alessandro Pignatti, Mauro Manno","doi":"10.1055/a-2441-2543","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background and study aims</b> Colorectal endoscopic submucosal dissection (ESD) is often challenging and time-consuming. Prolonged sedation and general anesthesia are associated with a relevant risk of anesthesia-related adverse events (ARAEs), especially in elderly and frail patients. Spinal anesthesia (SA), a simple technique providing analgesia and motor block without systemic drug administration, has never been described in gastrointestinal endoscopy. We assessed the feasibility of SA in colorectal lesion ESD. <b>Patients and methods</b> We retrospectively collected data on all consecutive patients who underwent ESD for colorectal laterally spreading tumors (LSTs) under SA in our center during the last 3 years. We evaluated the rates of technical success, i.e. ESD completion under SA without need of conversion to deep sedation or general anesthesia, and ARAEs after SA. <b>Results</b> ESD under SA was performed on 20 rectosigmoid LSTs ≥ 35 mm. Technical success was achieved in 95.0% of cases (19/20), while one patient (5.0%) required conversion to deep sedation. Two patients (10.0%) experienced acute urinary retention that was successfully treated with temporary catheterization. <b>Conclusions</b> Our initial experience suggests that SA for ESD of large rectosigmoid LSTs is feasible, and it may prove to be a valuable option, especially for elderly and frail patients.</p>","PeriodicalId":11671,"journal":{"name":"Endoscopy International Open","volume":"12 12","pages":"E1447-E1452"},"PeriodicalIF":2.3000,"publicationDate":"2024-12-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11651919/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endoscopy International Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2441-2543","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
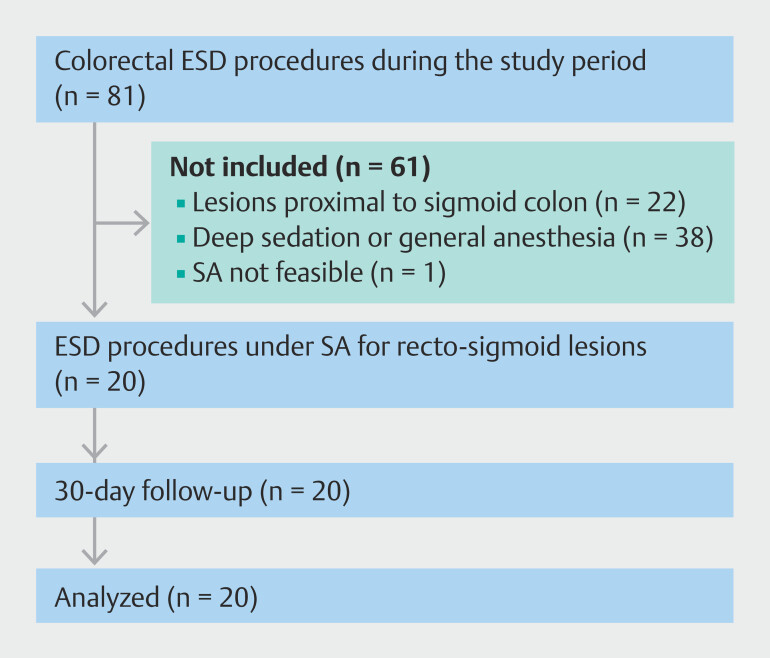
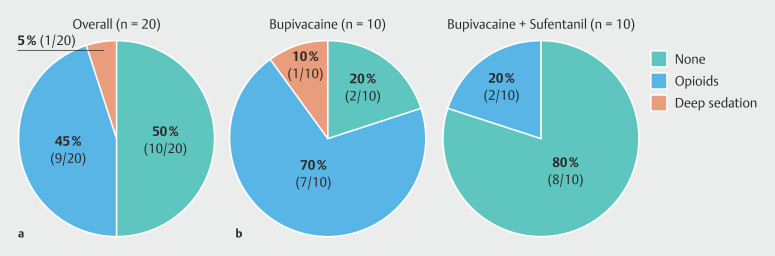
Background and study aims Colorectal endoscopic submucosal dissection (ESD) is often challenging and time-consuming. Prolonged sedation and general anesthesia are associated with a relevant risk of anesthesia-related adverse events (ARAEs), especially in elderly and frail patients. Spinal anesthesia (SA), a simple technique providing analgesia and motor block without systemic drug administration, has never been described in gastrointestinal endoscopy. We assessed the feasibility of SA in colorectal lesion ESD. Patients and methods We retrospectively collected data on all consecutive patients who underwent ESD for colorectal laterally spreading tumors (LSTs) under SA in our center during the last 3 years. We evaluated the rates of technical success, i.e. ESD completion under SA without need of conversion to deep sedation or general anesthesia, and ARAEs after SA. Results ESD under SA was performed on 20 rectosigmoid LSTs ≥ 35 mm. Technical success was achieved in 95.0% of cases (19/20), while one patient (5.0%) required conversion to deep sedation. Two patients (10.0%) experienced acute urinary retention that was successfully treated with temporary catheterization. Conclusions Our initial experience suggests that SA for ESD of large rectosigmoid LSTs is feasible, and it may prove to be a valuable option, especially for elderly and frail patients.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
