Padam Kanta Dahal, Zanfina Ademi, Lal Rawal, Rashidul Alam Mahumud, Grish Paudel, Biraj Karmacharya, Haruka Sakamoto, Tomohiko Sugishita, Corneel Vandelanotte
{"title":"Health economic evaluation alongside randomised clinical trial of a health behaviour intervention to manage type 2 diabetes in Nepal.","authors":"Padam Kanta Dahal, Zanfina Ademi, Lal Rawal, Rashidul Alam Mahumud, Grish Paudel, Biraj Karmacharya, Haruka Sakamoto, Tomohiko Sugishita, Corneel Vandelanotte","doi":"10.1186/s41256-024-00364-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prevention of type 2 diabetes is becoming an urgent public health concern in low and middle-income countries (LMICs). However, there is currently no evidence of a cost-effective approach of health behaviour interventions from community settings in low-income countries like Nepal. Therefore, this study aimed to assess the within-trial economic evaluation of a health behaviour intervention compared with usual care for managing type 2 diabetes in a community setting in Nepal.</p><p><strong>Methods: </strong>We randomly assigned 30 clusters comprising 481 patients with type 2 diabetes of which 15 to a health behaviour intervention (n = 238 patients) and 15 to the usual care (n = 243 patients). Patients in the intervention group received community health workers-led intensive training for diabetes self-management along with regular phone calls and ongoing support from peer supporters. Costs, quality-adjusted life years (QALYs) and incremental cost-effectiveness ratio (ICER) as costs per QALYs gained were assessed after 6-month from a healthcare system perspective. Probabilistic sensitivity analysis was conducted using 10,000 Monte Carlo simulations to assess the impact of uncertainty of cost-effectiveness analysis under the threshold of three times gross domestic product (GDP) per capita for Nepal (i.e., US $4,140).</p><p><strong>Results: </strong>Over the 6-month, the intervention yielded an incremental cost of US $28.55 (95% CI = US $21.26 to US $35.84) per person and an incremental QALYs of 0.0085 (95% CI = -0.0106 to 0.0275) per person. The ICER associated with the health behaviour intervention was US $3,358.82 (95% CI = US $-2005.66 to US $3,974.54) per QALY gained, which was below the estimated threshold, indicating a cost-effective approach with a net monetary benefit of US $6.64 (95% CI = US $-22.62 to US $78.01). Furthermore, the probabilistic sensitivity analysis consisting of 10,000 Monte Carlo simulations indicates that the intervention being cost-effective at the given threshold was 89.63%.</p><p><strong>Conclusions: </strong>Health behaviour interventions in community settings are a cost-effective approach to manage type 2 diabetes, offering good value for money. However, more studies focused on long-term follow-up across diverse setting of LMICs should be warranted to assess the maximum impact of such interventions.</p><p><strong>Trial registration: </strong>Australia and New Zealand Clinical Trial Registry (ACTRN12621000531819) Registered on 6<sup>th</sup> May 2021.</p>","PeriodicalId":52405,"journal":{"name":"Global Health Research and Policy","volume":"9 1","pages":"52"},"PeriodicalIF":4.6000,"publicationDate":"2024-12-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11650842/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Health Research and Policy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s41256-024-00364-z","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Prevention of type 2 diabetes is becoming an urgent public health concern in low and middle-income countries (LMICs). However, there is currently no evidence of a cost-effective approach of health behaviour interventions from community settings in low-income countries like Nepal. Therefore, this study aimed to assess the within-trial economic evaluation of a health behaviour intervention compared with usual care for managing type 2 diabetes in a community setting in Nepal.
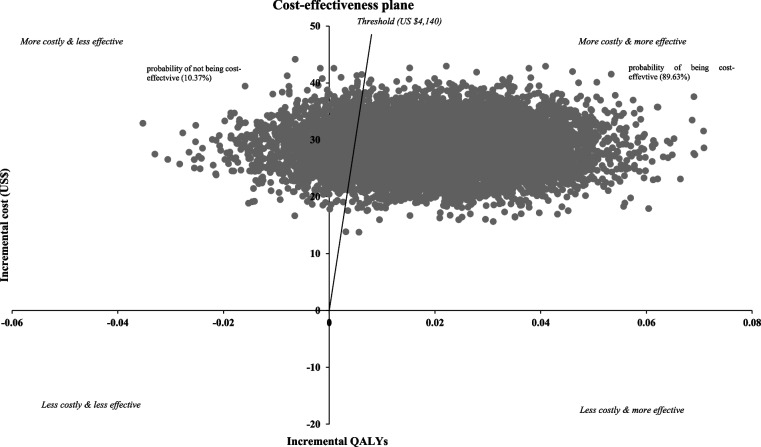
Methods: We randomly assigned 30 clusters comprising 481 patients with type 2 diabetes of which 15 to a health behaviour intervention (n = 238 patients) and 15 to the usual care (n = 243 patients). Patients in the intervention group received community health workers-led intensive training for diabetes self-management along with regular phone calls and ongoing support from peer supporters. Costs, quality-adjusted life years (QALYs) and incremental cost-effectiveness ratio (ICER) as costs per QALYs gained were assessed after 6-month from a healthcare system perspective. Probabilistic sensitivity analysis was conducted using 10,000 Monte Carlo simulations to assess the impact of uncertainty of cost-effectiveness analysis under the threshold of three times gross domestic product (GDP) per capita for Nepal (i.e., US $4,140).
Results: Over the 6-month, the intervention yielded an incremental cost of US $28.55 (95% CI = US $21.26 to US $35.84) per person and an incremental QALYs of 0.0085 (95% CI = -0.0106 to 0.0275) per person. The ICER associated with the health behaviour intervention was US $3,358.82 (95% CI = US $-2005.66 to US $3,974.54) per QALY gained, which was below the estimated threshold, indicating a cost-effective approach with a net monetary benefit of US $6.64 (95% CI = US $-22.62 to US $78.01). Furthermore, the probabilistic sensitivity analysis consisting of 10,000 Monte Carlo simulations indicates that the intervention being cost-effective at the given threshold was 89.63%.
Conclusions: Health behaviour interventions in community settings are a cost-effective approach to manage type 2 diabetes, offering good value for money. However, more studies focused on long-term follow-up across diverse setting of LMICs should be warranted to assess the maximum impact of such interventions.
Trial registration: Australia and New Zealand Clinical Trial Registry (ACTRN12621000531819) Registered on 6th May 2021.
背景:2型糖尿病的预防正在成为低收入和中等收入国家(LMICs)迫切关注的公共卫生问题。然而,目前没有证据表明,在尼泊尔等低收入国家的社区环境中,有一种具有成本效益的卫生行为干预方法。因此,本研究旨在评估尼泊尔社区环境中健康行为干预与常规护理管理2型糖尿病的试验内经济评估。方法:我们随机分配30组481例2型糖尿病患者,其中15例进行健康行为干预(n = 238例),15例进行常规护理(n = 243例)。干预组的患者接受了社区卫生工作者领导的糖尿病自我管理强化培训,并定期打电话和同伴支持者的持续支持。6个月后从医疗保健系统的角度评估成本、质量调整生命年(QALYs)和增量成本效益比(ICER),即每个QALYs获得的成本。使用10,000个蒙特卡罗模拟进行了概率敏感性分析,以评估尼泊尔人均国内生产总值(GDP)三倍(即4,140美元)阈值下成本效益分析的不确定性的影响。结果:在6个月的时间里,干预产生了每人28.55美元的增量成本(95% CI = 21.26至35.84美元)和每人0.0085美元的增量质量年(95% CI = -0.0106至0.0275)。与健康行为干预相关的ICER为每QALY获得3,358.82美元(95% CI = -2005.66美元至3,974.54美元),低于估计阈值,表明该方法具有成本效益,净货币效益为6.64美元(95% CI = -22.62美元至78.01美元)。此外,由10,000个蒙特卡罗模拟组成的概率敏感性分析表明,在给定阈值下,干预措施的成本效益为89.63%。结论:社区环境中的健康行为干预是管理2型糖尿病的一种具有成本效益的方法,物有所值。然而,为了评估这些干预措施的最大影响,有必要开展更多的研究,重点关注不同低收入国家的长期随访。试验注册:澳大利亚和新西兰临床试验注册中心(ACTRN12621000531819)于2021年5月6日注册。
期刊介绍:
Global Health Research and Policy, an open-access, multidisciplinary journal, publishes research on various aspects of global health, addressing topics like health equity, health systems and policy, social determinants of health, disease burden, population health, and other urgent global health issues. It serves as a forum for high-quality research focused on regional and global health improvement, emphasizing solutions for health equity.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
