Joel Li Ji Chin, Yu Guang Tan, Alvin Wei Xiang Low, Kenneth Chen, Henry Sun Sien Ho, Christopher Wai Sam Cheng, John Shyi Peng Yuen, Kae Jack Tay
{"title":"Unravelling the natural history of localised prostate cancer in the post-prostate specific antigen era: implications for clinical management.","authors":"Joel Li Ji Chin, Yu Guang Tan, Alvin Wei Xiang Low, Kenneth Chen, Henry Sun Sien Ho, Christopher Wai Sam Cheng, John Shyi Peng Yuen, Kae Jack Tay","doi":"10.21037/tau-24-322","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Management of localised prostate cancer (PCa) remains controversial in the era of prostate-specific antigen (PSA) testing. This study aims to describe the natural history of men with PCa being followed up expectantly to evaluate disease mortality.</p><p><strong>Methods: </strong>After exclusion, clinical data of 204 patients retrieved from a prospective large PCa registry were reviewed. Competing risk analysis were performed using the Fine-Gray model.</p><p><strong>Results: </strong>The median age was 73 years old with a median follow up of 12.5 years. The median PSA was 8.85 ng/mL and the risk stratification were as follows: low (47.0%), intermediate (31.4%), and high risk (21.6%). There were 19 PCa (9.3%) and 84 non-PCa deaths (41.2%), with overall mortality at 50.5%. Multivariate analysis showed patients with high PSA values [subdistribution hazard ratio (sdHR) 7.13], poorer prostate cancer grade groups (PCGG) (sdHR 16.349), and therefore higher European Association of Urology risk group (sdHR 11.42) had greatly elevated prostate cancer mortality (PCM). Older patients greater than 75 years of age (sdHR 4.52) and high Charlson Comorbidity Index (CCI ≥6) scores had higher non-prostate cancer mortality (NPCM) (sdHR 7.87). Subgroup analysis of the high-risk group showed having a lower CCI score (≤3) had a greater risk of PCM than NPCM (sdHR 4.31 <i>vs.</i> 0.22) while the converse is observed for higher CCI scores (1.12 <i>vs.</i> 5.52).</p><p><strong>Conclusions: </strong>Overall PCM remains low in elderly men with conservatively treated PCa. Age and poorer CCI predict NPCM while PSA and PCGG predict PCM. In high-risk PCa group, CCI is a useful tool to determine which patients will benefit from radical treatment.</p>","PeriodicalId":23270,"journal":{"name":"Translational andrology and urology","volume":"13 11","pages":"2459-2467"},"PeriodicalIF":1.7000,"publicationDate":"2024-11-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11650342/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational andrology and urology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tau-24-322","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/27 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ANDROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Management of localised prostate cancer (PCa) remains controversial in the era of prostate-specific antigen (PSA) testing. This study aims to describe the natural history of men with PCa being followed up expectantly to evaluate disease mortality.
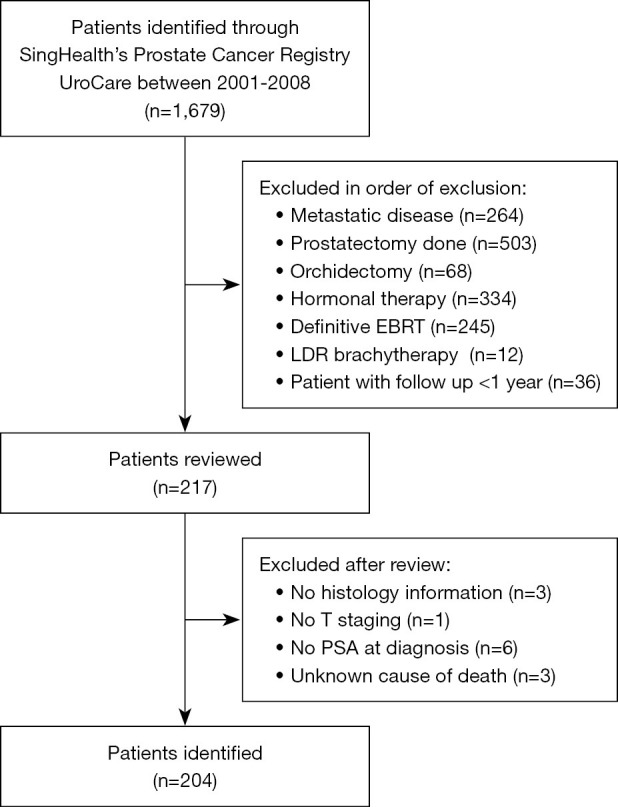
Methods: After exclusion, clinical data of 204 patients retrieved from a prospective large PCa registry were reviewed. Competing risk analysis were performed using the Fine-Gray model.
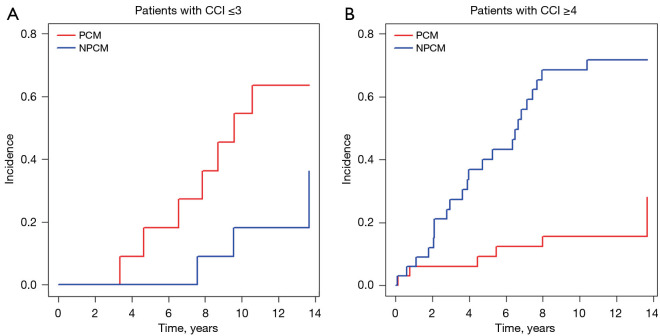
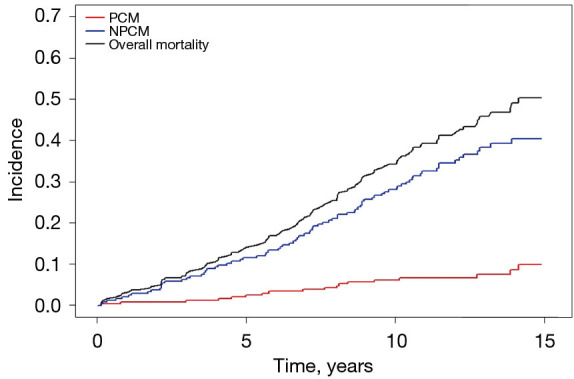
Results: The median age was 73 years old with a median follow up of 12.5 years. The median PSA was 8.85 ng/mL and the risk stratification were as follows: low (47.0%), intermediate (31.4%), and high risk (21.6%). There were 19 PCa (9.3%) and 84 non-PCa deaths (41.2%), with overall mortality at 50.5%. Multivariate analysis showed patients with high PSA values [subdistribution hazard ratio (sdHR) 7.13], poorer prostate cancer grade groups (PCGG) (sdHR 16.349), and therefore higher European Association of Urology risk group (sdHR 11.42) had greatly elevated prostate cancer mortality (PCM). Older patients greater than 75 years of age (sdHR 4.52) and high Charlson Comorbidity Index (CCI ≥6) scores had higher non-prostate cancer mortality (NPCM) (sdHR 7.87). Subgroup analysis of the high-risk group showed having a lower CCI score (≤3) had a greater risk of PCM than NPCM (sdHR 4.31 vs. 0.22) while the converse is observed for higher CCI scores (1.12 vs. 5.52).
Conclusions: Overall PCM remains low in elderly men with conservatively treated PCa. Age and poorer CCI predict NPCM while PSA and PCGG predict PCM. In high-risk PCa group, CCI is a useful tool to determine which patients will benefit from radical treatment.
期刊介绍:
ranslational Andrology and Urology (Print ISSN 2223-4683; Online ISSN 2223-4691; Transl Androl Urol; TAU) is an open access, peer-reviewed, bi-monthly journal (quarterly published from Mar.2012 - Dec. 2014). The main focus of the journal is to describe new findings in the field of translational research of Andrology and Urology, provides current and practical information on basic research and clinical investigations of Andrology and Urology. Specific areas of interest include, but not limited to, molecular study, pathology, biology and technical advances related to andrology and urology. Topics cover range from evaluation, prevention, diagnosis, therapy, prognosis, rehabilitation and future challenges to urology and andrology. Contributions pertinent to urology and andrology are also included from related fields such as public health, basic sciences, education, sociology, and nursing.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
