{"title":"LONG-TERM SURVIVAL AFTER LAPAROSCOPIC TOTAL GASTRECTOMY FOR EARLY AND ADVANCED GASTRIC CANCER. SINGLE CENTER EXPERIENCE IN 100 CASES.","authors":"Enrique Norero, Marco Ceroni, Cristian Martinez, Rodrigo Muñoz, Ricardo Mejia, Emilio Morales, Ignacio Obaid, Paulina Gonzalez","doi":"10.1590/0102-6720202400050e1844","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Laparoscopic gastrectomy offers advantages in the postoperative period compared to the open approach. Most studies have been performed on distal gastrectomies; however, laparoscopic total gastrectomy (LTG) is not universally accepted. AIM: The aim of this study was to assess the results of LTG, on postoperative morbidity outcomes and long-term survival.</p><p><strong>Methods: </strong>This is a retrospective cohort study from a prospective database of patients who underwent LTG, from 2005 to 2022, due to early and advanced gastric cancer. A totally laparoscopic technique was utilized, and the Roux-en-Y reconstruction was performed in all cases. Postoperative complications and long-term survival were evaluated.</p><p><strong>Results: </strong>A total of 100 patients were included (men 57, age 64 years, and body mass index 26). A D2 lymphadenectomy was performed in 68 cases. The postoperative hospitalization period was 8 days (6-62 days). Postoperative complications occurred in 26%, with 7% esophago-jejunal anastomosis leak, 4% abdominal collections, and 2% gastrointestinal bleeding. In 7% of cases, the complication was considered Clavien 3 or greater. Operative mortality was 1%. The pathology findings confirmed advanced gastric cancer in 50 cases. The median lymph node count was 38, and surgery was considered R0 in 99%. The median follow-up was 50 months. Overall 5-year survival was 74%. Survival in T1 cases was 95% at 5 years. For stage I, survival was 95%, and for stages II and III, it was 52% and 43%, at 5 years, respectively.</p><p><strong>Conclusions: </strong>These results support the feasibility and oncological adequacy of minimally invasive total gastrectomy. Postoperative morbidity has an acceptable rate. Long-term survival was in accordance with the disease stage.</p>","PeriodicalId":72298,"journal":{"name":"Arquivos brasileiros de cirurgia digestiva : ABCD = Brazilian archives of digestive surgery","volume":"37 ","pages":"e1844"},"PeriodicalIF":1.8000,"publicationDate":"2024-12-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11655072/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arquivos brasileiros de cirurgia digestiva : ABCD = Brazilian archives of digestive surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1590/0102-6720202400050e1844","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Laparoscopic gastrectomy offers advantages in the postoperative period compared to the open approach. Most studies have been performed on distal gastrectomies; however, laparoscopic total gastrectomy (LTG) is not universally accepted. AIM: The aim of this study was to assess the results of LTG, on postoperative morbidity outcomes and long-term survival.
Methods: This is a retrospective cohort study from a prospective database of patients who underwent LTG, from 2005 to 2022, due to early and advanced gastric cancer. A totally laparoscopic technique was utilized, and the Roux-en-Y reconstruction was performed in all cases. Postoperative complications and long-term survival were evaluated.
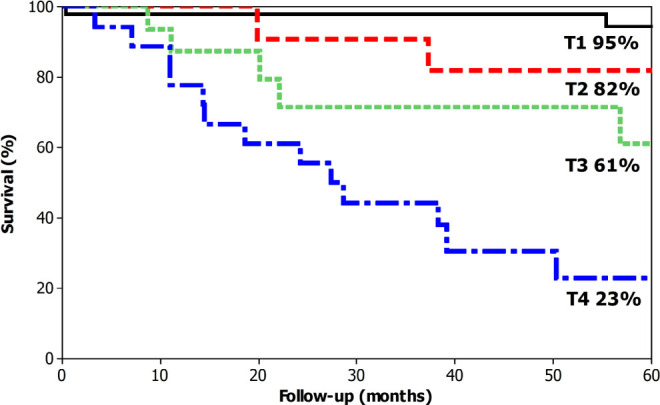
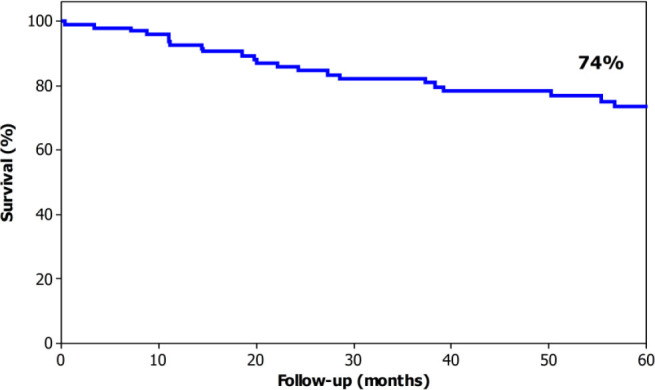
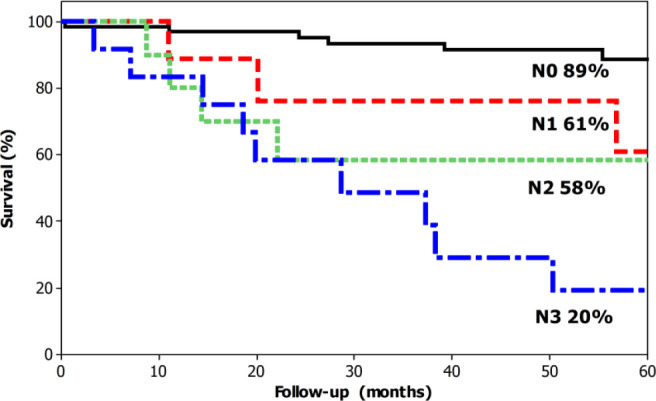
Results: A total of 100 patients were included (men 57, age 64 years, and body mass index 26). A D2 lymphadenectomy was performed in 68 cases. The postoperative hospitalization period was 8 days (6-62 days). Postoperative complications occurred in 26%, with 7% esophago-jejunal anastomosis leak, 4% abdominal collections, and 2% gastrointestinal bleeding. In 7% of cases, the complication was considered Clavien 3 or greater. Operative mortality was 1%. The pathology findings confirmed advanced gastric cancer in 50 cases. The median lymph node count was 38, and surgery was considered R0 in 99%. The median follow-up was 50 months. Overall 5-year survival was 74%. Survival in T1 cases was 95% at 5 years. For stage I, survival was 95%, and for stages II and III, it was 52% and 43%, at 5 years, respectively.
Conclusions: These results support the feasibility and oncological adequacy of minimally invasive total gastrectomy. Postoperative morbidity has an acceptable rate. Long-term survival was in accordance with the disease stage.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
