Effect of External Beam Radiation Therapy and Brachytherapy on Circulating Myeloid-Derived Suppressor Cell Populations in Patients Treated Definitively for Cervical Cancer
Kelsey M. Wanhainen MD, PhD , Matthew Berkseth PhD , Nicole Sando BS , Lydia Golden BS , Amy Techam RN, PHN , Jennifer Wieworka DNP , Kyra M. Boorsma Bergerud BS , Peter Argenta MD , Andrea O'Shea MD , Britt K. Erickson MD , Sally Mullany MD , Colleen Rivard MD , Rahel Ghebre MD, MPH , Deanna Teoh MD, MS , Margaret Reynolds MD , Stephanie Terezakis MD , Jianling Yuan MD, PhD , Lindsey Sloan MD, PhD
{"title":"Effect of External Beam Radiation Therapy and Brachytherapy on Circulating Myeloid-Derived Suppressor Cell Populations in Patients Treated Definitively for Cervical Cancer","authors":"Kelsey M. Wanhainen MD, PhD , Matthew Berkseth PhD , Nicole Sando BS , Lydia Golden BS , Amy Techam RN, PHN , Jennifer Wieworka DNP , Kyra M. Boorsma Bergerud BS , Peter Argenta MD , Andrea O'Shea MD , Britt K. Erickson MD , Sally Mullany MD , Colleen Rivard MD , Rahel Ghebre MD, MPH , Deanna Teoh MD, MS , Margaret Reynolds MD , Stephanie Terezakis MD , Jianling Yuan MD, PhD , Lindsey Sloan MD, PhD","doi":"10.1016/j.adro.2024.101677","DOIUrl":null,"url":null,"abstract":"<div><h3>Purpose</h3><div>The immunosuppressive function of myeloid-derived suppressor cells (MDSCs) has been implicated in the regulation of immune responses against cancer and is associated with poor prognosis. Radiation treatment is known to alter immune cell populations within the tumor; however, whether this results in the recruitment of immunosuppressive MDSC populations is not well understood. Here we evaluate the response of circulating MDSC populations in patients treated per standard-of-care cisplatin chemoradiation therapy (CRT) for locally invasive cervical cancer.</div></div><div><h3>Methods and Materials</h3><div>Newly diagnosed, treatment-naïve patients with locally advanced cervical cancer were enrolled. Blood samples were collected from patients prior to starting CRT (T<sub>0</sub>), after external beam radiation therapy (T<sub>1</sub>), and after high-dose-rate brachytherapy (T<sub>2</sub>). Samples from each time point were processed, and the prevalence of MDSC subsets was determined using flow cytometry. MDSC populations were identified using Live/Dead-CD11b+CD33+HLA-DR- staining. MDSC subsets were further subdivided into granulocytic (g-, CD15+CD14-), monocytic (m-, CD15-CD14+), or early-MDSCs (e-, CD15-CD14-).</div></div><div><h3>Results</h3><div>Most patients in our study were Caucasian nonsmokers with human papillomavirus-associated squamous cell carcinoma of the cervix. We saw a trend for increased MDSC frequency in patients with more advanced-stage disease at the time of initiating treatment. MDSCs increase in response to CRT and peak after brachytherapy (T<sub>2</sub>). In particular, the g-MDSC subset increases by 6.44 times relative to the baseline. There was no correlation between MDSC expansion and response to therapy.</div></div><div><h3>Conclusion</h3><div>Our study confirms other reports that circulating MDSCs in patients with cervical cancer increase in response to CRT and are associated with more advanced stages. Additionally, we show that MDSC expansion is driven by the g-MDSC subset. We did not see any correlation between MDSC expansion and treatment response, though this may be because of the limited sample size for this study.</div></div>","PeriodicalId":7390,"journal":{"name":"Advances in Radiation Oncology","volume":"10 2","pages":"Article 101677"},"PeriodicalIF":2.7000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11653128/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Radiation Oncology","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2452109424002409","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/14 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose
The immunosuppressive function of myeloid-derived suppressor cells (MDSCs) has been implicated in the regulation of immune responses against cancer and is associated with poor prognosis. Radiation treatment is known to alter immune cell populations within the tumor; however, whether this results in the recruitment of immunosuppressive MDSC populations is not well understood. Here we evaluate the response of circulating MDSC populations in patients treated per standard-of-care cisplatin chemoradiation therapy (CRT) for locally invasive cervical cancer.
Methods and Materials
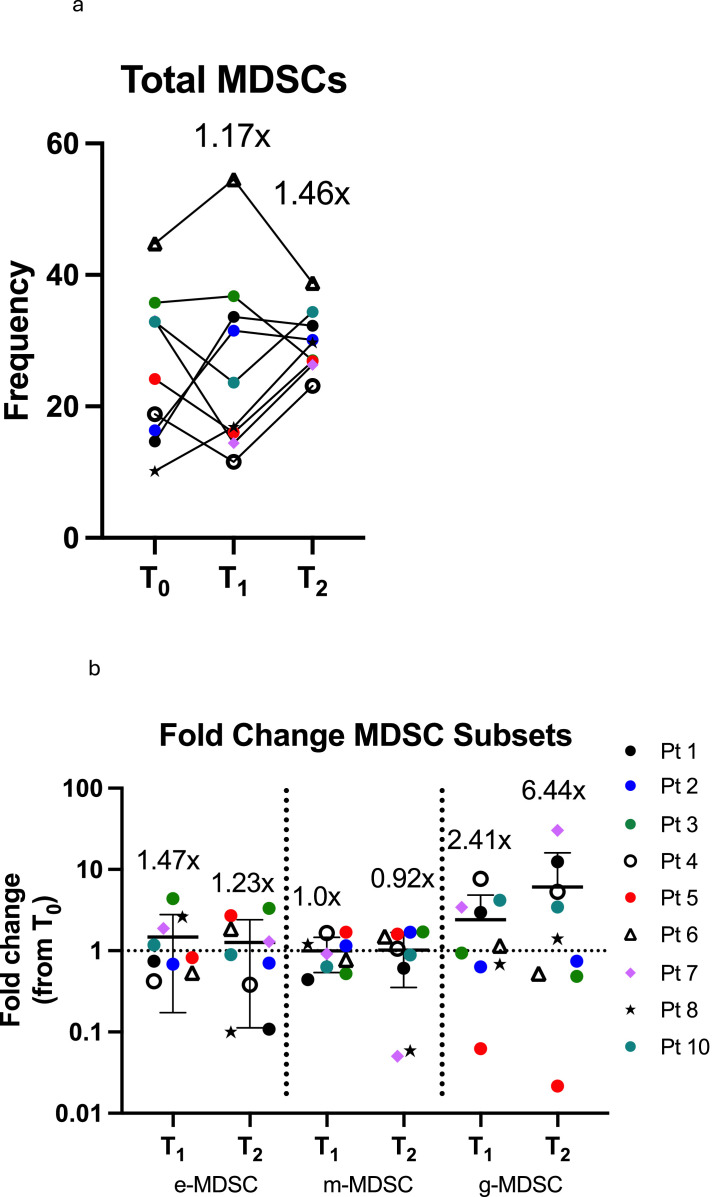
Newly diagnosed, treatment-naïve patients with locally advanced cervical cancer were enrolled. Blood samples were collected from patients prior to starting CRT (T0), after external beam radiation therapy (T1), and after high-dose-rate brachytherapy (T2). Samples from each time point were processed, and the prevalence of MDSC subsets was determined using flow cytometry. MDSC populations were identified using Live/Dead-CD11b+CD33+HLA-DR- staining. MDSC subsets were further subdivided into granulocytic (g-, CD15+CD14-), monocytic (m-, CD15-CD14+), or early-MDSCs (e-, CD15-CD14-).
Results
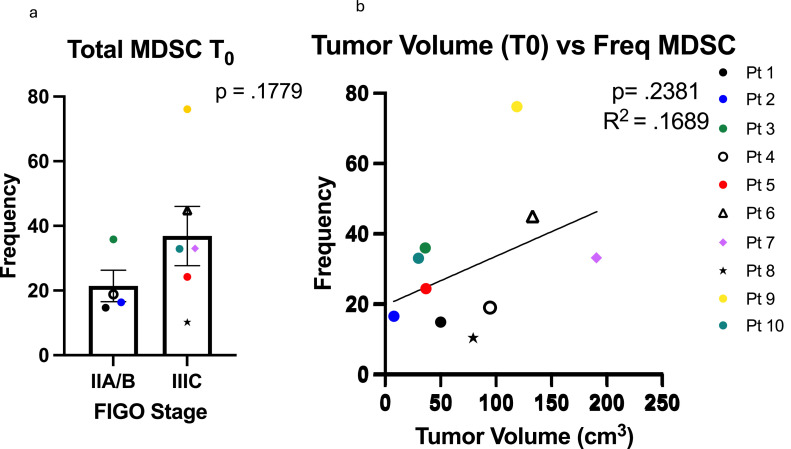
Most patients in our study were Caucasian nonsmokers with human papillomavirus-associated squamous cell carcinoma of the cervix. We saw a trend for increased MDSC frequency in patients with more advanced-stage disease at the time of initiating treatment. MDSCs increase in response to CRT and peak after brachytherapy (T2). In particular, the g-MDSC subset increases by 6.44 times relative to the baseline. There was no correlation between MDSC expansion and response to therapy.
Conclusion
Our study confirms other reports that circulating MDSCs in patients with cervical cancer increase in response to CRT and are associated with more advanced stages. Additionally, we show that MDSC expansion is driven by the g-MDSC subset. We did not see any correlation between MDSC expansion and treatment response, though this may be because of the limited sample size for this study.
期刊介绍:
The purpose of Advances is to provide information for clinicians who use radiation therapy by publishing: Clinical trial reports and reanalyses. Basic science original reports. Manuscripts examining health services research, comparative and cost effectiveness research, and systematic reviews. Case reports documenting unusual problems and solutions. High quality multi and single institutional series, as well as other novel retrospective hypothesis generating series. Timely critical reviews on important topics in radiation oncology, such as side effects. Articles reporting the natural history of disease and patterns of failure, particularly as they relate to treatment volume delineation. Articles on safety and quality in radiation therapy. Essays on clinical experience. Articles on practice transformation in radiation oncology, in particular: Aspects of health policy that may impact the future practice of radiation oncology. How information technology, such as data analytics and systems innovations, will change radiation oncology practice. Articles on imaging as they relate to radiation therapy treatment.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
