{"title":"Pregnancy-Related Morphea: A Case Report.","authors":"Sedigheh Borna, Zeynab Zamanpour, Safoura Shakoei, Maryam Aliasgharpoor, Zahra Hamidi Madani","doi":"10.1177/11795476241302563","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Morphea is a skin condition marked by erythematous and hardened inflammatory lesions that can progress to atrophic and sclerotic plaques. In this case report, we present a case of a pregnant woman who showed morphea presentation.</p><p><strong>Case presentation: </strong>A 37-year-old G<sub>2</sub>P<sub>1</sub>L<sub>1</sub> woman with a gestational age of 32 weeks and 2 days was referred to the hospital with complaints of swelling, pain, and erythema in both legs for the past week, without any obstetric complaints. Upon initial examination at the time of admission, swelling, erythema, warmth in both legs, ecchymotic lesions, and non-pitting edema were observed. Biometry and color Doppler ultrasound for evaluation of fetus growth was normal. Skin examination revealed mild erythema, warmth, and purpura and petechiae in some areas, with an orange peel appearance and firm texture on palpation. Leg lesion skin punch biopsy reported a sclerodermoid reaction pattern and findings more compatible with morphea. The patient was managed for morphea during pregnancy. However, at 38 weeks and 6 days of gestation, due to worsening symptoms and spreading stiffness to the groin area, and the need for initiating pulse corticosteroids and mycophenolate mofetil (CellCept), the patient was re-admitted for cesarean section. In the follow-up assessment, ultrasound findings were normal, IGRA, HIV antibody, HCV antibody, HBC antigen, and HBS antigen were negative, and no edema or inflammation was seen in the patient.</p><p><strong>Conclusions: </strong>In conclusion, although our patient recovered without specific treatment, predicting the recurrence or worsening of morphea in future pregnancies is challenging.</p>","PeriodicalId":10357,"journal":{"name":"Clinical Medicine Insights. Case Reports","volume":"17 ","pages":"11795476241302563"},"PeriodicalIF":0.6000,"publicationDate":"2024-12-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11656421/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795476241302563","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Morphea is a skin condition marked by erythematous and hardened inflammatory lesions that can progress to atrophic and sclerotic plaques. In this case report, we present a case of a pregnant woman who showed morphea presentation.
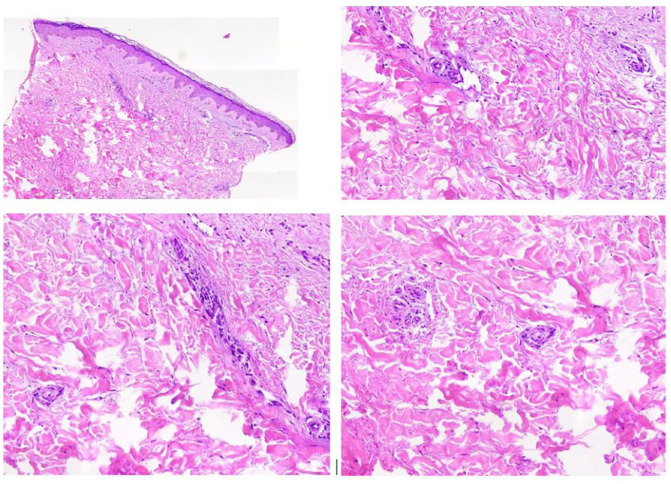
Case presentation: A 37-year-old G2P1L1 woman with a gestational age of 32 weeks and 2 days was referred to the hospital with complaints of swelling, pain, and erythema in both legs for the past week, without any obstetric complaints. Upon initial examination at the time of admission, swelling, erythema, warmth in both legs, ecchymotic lesions, and non-pitting edema were observed. Biometry and color Doppler ultrasound for evaluation of fetus growth was normal. Skin examination revealed mild erythema, warmth, and purpura and petechiae in some areas, with an orange peel appearance and firm texture on palpation. Leg lesion skin punch biopsy reported a sclerodermoid reaction pattern and findings more compatible with morphea. The patient was managed for morphea during pregnancy. However, at 38 weeks and 6 days of gestation, due to worsening symptoms and spreading stiffness to the groin area, and the need for initiating pulse corticosteroids and mycophenolate mofetil (CellCept), the patient was re-admitted for cesarean section. In the follow-up assessment, ultrasound findings were normal, IGRA, HIV antibody, HCV antibody, HBC antigen, and HBS antigen were negative, and no edema or inflammation was seen in the patient.
Conclusions: In conclusion, although our patient recovered without specific treatment, predicting the recurrence or worsening of morphea in future pregnancies is challenging.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
