Eris van Twist, Tahisa B Robles, Bart Formsma, Naomi Ketharanathan, Maayke Hunfeld, C M Buysse, Matthijs de Hoog, Alfred C Schouten, Rogier C J de Jonge, Jan W Kuiper
{"title":"An open source autoregulation-based neuromonitoring algorithm shows PRx and optimal CPP association with pediatric traumatic brain injury.","authors":"Eris van Twist, Tahisa B Robles, Bart Formsma, Naomi Ketharanathan, Maayke Hunfeld, C M Buysse, Matthijs de Hoog, Alfred C Schouten, Rogier C J de Jonge, Jan W Kuiper","doi":"10.1007/s10877-024-01248-w","DOIUrl":null,"url":null,"abstract":"<p><p>This study aimed to develop an open-source algorithm for the pressure-reactivity index (PRx) to monitor cerebral autoregulation (CA) in pediatric severe traumatic brain injury (sTBI) and compared derived optimal cerebral perfusion pressure (CPPopt) with real-time CPP in relation to long-term outcome. Retrospective study in children (< 18 years) with sTBI admitted to the pediatric intensive care unit (PICU) for intracranial pressure (ICP) monitoring between 2016 and 2023. ICP was analyzed on an insult basis and correlated with outcome. PRx was calculated as Pearson correlation coefficient between ICP and mean arterial pressure. CPPopt was derived as weighted average of CPP-PRx over time. Outcome was determined via Pediatric Cerebral Performance Category (PCPC) scale at one year post-injury. Logistic regression and mixed effect models were developed to associate PRx and CPPopt with outcome. In total 50 children were included, 35 with favorable (PCPC 1-3) and 15 with unfavorable outcome (PCPC 4-6). ICP insults correlated with unfavorable outcome at 20 mmHg for 7 min duration. Mean CPPopt yield was 75.4% of monitoring time. Mean and median PRx and CPPopt yield associated with unfavorable outcome, with odds ratio (OR) 2.49 (1.38-4.50), 1.38 (1.08-1.76) and 0.95 (0.92-0.97) (p < 0.001). PRx thresholds 0.0, 0.20, 0.25 and 0.30 resulted in OR 1.01 (1.00-1.02) (p < 0.006). CPP in optimal range associated with unfavorable outcome on day one (0.018, p = 0.029) and four (-0.026, p = 0.025). Our algorithm can obtain optimal targets for pediatric neuromonitoring that showed association with long-term outcome, and is now available open source.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"291-299"},"PeriodicalIF":2.2000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12049323/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-024-01248-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/19 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
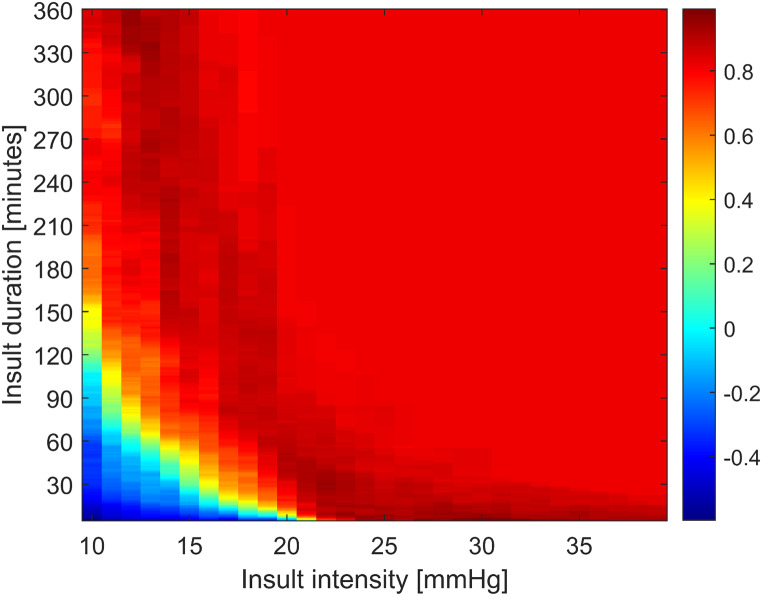
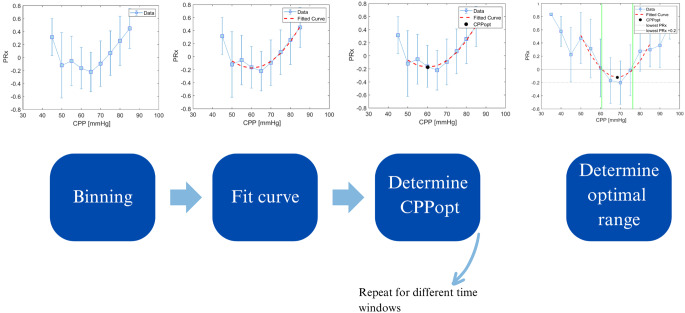
This study aimed to develop an open-source algorithm for the pressure-reactivity index (PRx) to monitor cerebral autoregulation (CA) in pediatric severe traumatic brain injury (sTBI) and compared derived optimal cerebral perfusion pressure (CPPopt) with real-time CPP in relation to long-term outcome. Retrospective study in children (< 18 years) with sTBI admitted to the pediatric intensive care unit (PICU) for intracranial pressure (ICP) monitoring between 2016 and 2023. ICP was analyzed on an insult basis and correlated with outcome. PRx was calculated as Pearson correlation coefficient between ICP and mean arterial pressure. CPPopt was derived as weighted average of CPP-PRx over time. Outcome was determined via Pediatric Cerebral Performance Category (PCPC) scale at one year post-injury. Logistic regression and mixed effect models were developed to associate PRx and CPPopt with outcome. In total 50 children were included, 35 with favorable (PCPC 1-3) and 15 with unfavorable outcome (PCPC 4-6). ICP insults correlated with unfavorable outcome at 20 mmHg for 7 min duration. Mean CPPopt yield was 75.4% of monitoring time. Mean and median PRx and CPPopt yield associated with unfavorable outcome, with odds ratio (OR) 2.49 (1.38-4.50), 1.38 (1.08-1.76) and 0.95 (0.92-0.97) (p < 0.001). PRx thresholds 0.0, 0.20, 0.25 and 0.30 resulted in OR 1.01 (1.00-1.02) (p < 0.006). CPP in optimal range associated with unfavorable outcome on day one (0.018, p = 0.029) and four (-0.026, p = 0.025). Our algorithm can obtain optimal targets for pediatric neuromonitoring that showed association with long-term outcome, and is now available open source.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
