{"title":"Uterine rupture with induction using misoprostol for intrauterine foetal death in the second trimester: A case report","authors":"Akiko Yamamoto, Patrick Jn-Charles","doi":"10.1016/j.crwh.2024.e00671","DOIUrl":null,"url":null,"abstract":"<div><div>Uterine rupture is a well-known, life-threatening complication of misoprostol use; the incidence is remarkably low. Herein, we report what seems to be the first documented case of uterine rupture following induction of labour for intrauterine foetal death in the second trimester without a uterine scar. A 40-year-old woman with no history of caesarean section or uterine surgery presented with mild lower abdominal pain and mild genital bleeding. Transabdominal ultrasonography revealed intrauterine foetal death, at presumed gestational age of 20 weeks. Two hours after three doses of 400 μg 3-hourly of misoprostol, the patient complained of abdominal pain; however, the foetus was not expelled. Repeat sonography revealed the foetus in the abdominal cavity and fluid collection in the pelvis. Based on the probable diagnosis of uterine rupture, a laparotomy was performed. The intra-abdominal haemorrhage volume was approximately 250–300 ml. There was a linear rupture approximately 10 cm long on the posterior wall of the uterus, and as a consequence, a macerated and foetid foetus and part of the placenta were found in the abdominal cavity. A total hysterectomy was performed, and the patient was discharged three days after the intervention without any postoperative complications. In conclusion, while misoprostol is generally safe for second-trimester pregnancy termination, its use should be approached with caution and close monitoring in cases of uterine inflammation.</div></div>","PeriodicalId":9657,"journal":{"name":"Case Reports in Women's Health","volume":"44 ","pages":"Article e00671"},"PeriodicalIF":0.6000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11665375/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Women's Health","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2214911224000924","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/30 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
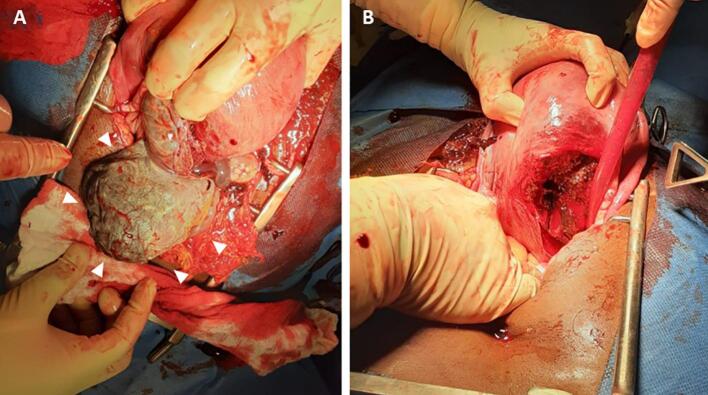
Uterine rupture is a well-known, life-threatening complication of misoprostol use; the incidence is remarkably low. Herein, we report what seems to be the first documented case of uterine rupture following induction of labour for intrauterine foetal death in the second trimester without a uterine scar. A 40-year-old woman with no history of caesarean section or uterine surgery presented with mild lower abdominal pain and mild genital bleeding. Transabdominal ultrasonography revealed intrauterine foetal death, at presumed gestational age of 20 weeks. Two hours after three doses of 400 μg 3-hourly of misoprostol, the patient complained of abdominal pain; however, the foetus was not expelled. Repeat sonography revealed the foetus in the abdominal cavity and fluid collection in the pelvis. Based on the probable diagnosis of uterine rupture, a laparotomy was performed. The intra-abdominal haemorrhage volume was approximately 250–300 ml. There was a linear rupture approximately 10 cm long on the posterior wall of the uterus, and as a consequence, a macerated and foetid foetus and part of the placenta were found in the abdominal cavity. A total hysterectomy was performed, and the patient was discharged three days after the intervention without any postoperative complications. In conclusion, while misoprostol is generally safe for second-trimester pregnancy termination, its use should be approached with caution and close monitoring in cases of uterine inflammation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
