Anh Tuan Le Truong, Hang Thi Minh Tran, Loc Dang Phan, Huong Bich Thi Nguyen, Trung Quoc Nguyen, Tra Vu Son Le, Duc Nguyen Chiem, Huy Nguyen, Thanh N Nguyen, Thang Huy Nguyen
{"title":"Predictive Value of the Prehospital RACE Scale for Large Vessel Occlusion in Acute Stroke Patients.","authors":"Anh Tuan Le Truong, Hang Thi Minh Tran, Loc Dang Phan, Huong Bich Thi Nguyen, Trung Quoc Nguyen, Tra Vu Son Le, Duc Nguyen Chiem, Huy Nguyen, Thanh N Nguyen, Thang Huy Nguyen","doi":"10.1159/000543260","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Prehospital stroke scales have been developed to identify anterior large vessel occlusion (LVO) in acute ischemic stroke (AIS) patients for direct transport to thrombectomy-capable hospitals. However, its performance in a Vietnamese population remains unknown. We aimed to evaluate the predictive value of the Rapid Arterial oCclusion Evaluation (RACE) scale for LVO detection in patients with ischemic stroke presenting within 24 h in Vietnam.</p><p><strong>Methods: </strong>This was a prospective study of patients with AIS admitted at People's 115 Hospital between May 2022 and October 2022. All patients were assessed with the RACE scale with five items: facial palsy (scored 0-2), arm motor function (0-2), leg motor function (0-2), gaze (0-1), and aphasia or agnosia (0-2). LVO was diagnosed by CTA or MRA. Receiver operating characteristic curve, sensitivity, specificity, and accuracy of the RACE scale were analyzed to evaluate its predictive value for LVO.</p><p><strong>Results: </strong>There were 318 patients included. LVO was detected in 121/318 patients (37.6%). The higher the RACE score, the higher the proportion of patients with LVO (p < 0.001). Receiver operating characteristic curves showed capacity to predict LVO of the RACE scale with an area under the curve (AUC) of 0.767. The optimal RACE cutoff was ≥5 with sensitivity = 0.68, specificity = 0.79, positive predictive value = 0.67, negative predictive value = 0.80, and overall accuracy = 0.75. RACE ≥5 had higher sensitivity and same specificity for detecting LVO in AIS patients within 6-h versus 6-24-h window (AUC = 0.79 vs. 0.75, sensitivity = 0.74 vs. 0.65, specificity = 0.79 vs. 0.80, accuracy = 0.77 vs. 0.74).</p><p><strong>Conclusions: </strong>The RACE scale is a simple tool that can accurately identify AIS patients with LVO. This tool may be useful for early detection of LVO patients and should be validated in the prehospital setting in Vietnam.</p>","PeriodicalId":45709,"journal":{"name":"Cerebrovascular Diseases Extra","volume":" ","pages":"39-47"},"PeriodicalIF":2.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11842085/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebrovascular Diseases Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000543260","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/24 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Prehospital stroke scales have been developed to identify anterior large vessel occlusion (LVO) in acute ischemic stroke (AIS) patients for direct transport to thrombectomy-capable hospitals. However, its performance in a Vietnamese population remains unknown. We aimed to evaluate the predictive value of the Rapid Arterial oCclusion Evaluation (RACE) scale for LVO detection in patients with ischemic stroke presenting within 24 h in Vietnam.
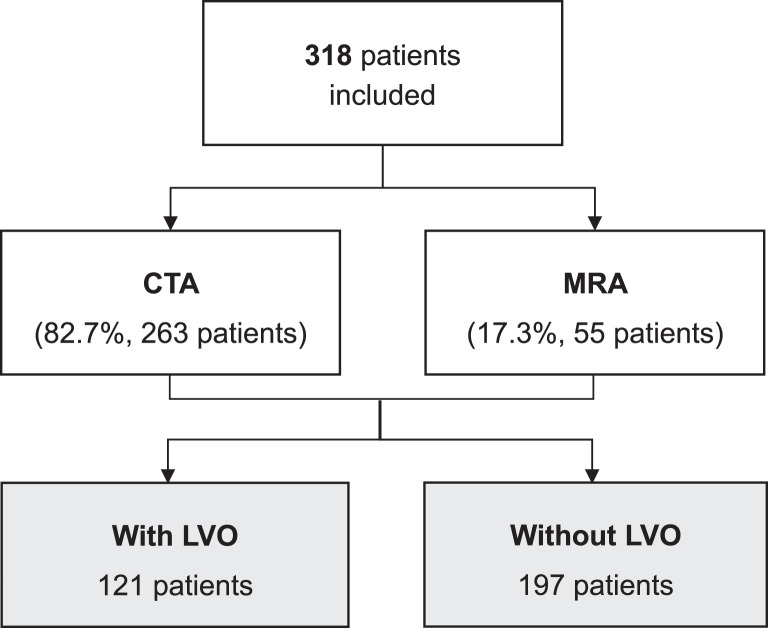
Methods: This was a prospective study of patients with AIS admitted at People's 115 Hospital between May 2022 and October 2022. All patients were assessed with the RACE scale with five items: facial palsy (scored 0-2), arm motor function (0-2), leg motor function (0-2), gaze (0-1), and aphasia or agnosia (0-2). LVO was diagnosed by CTA or MRA. Receiver operating characteristic curve, sensitivity, specificity, and accuracy of the RACE scale were analyzed to evaluate its predictive value for LVO.
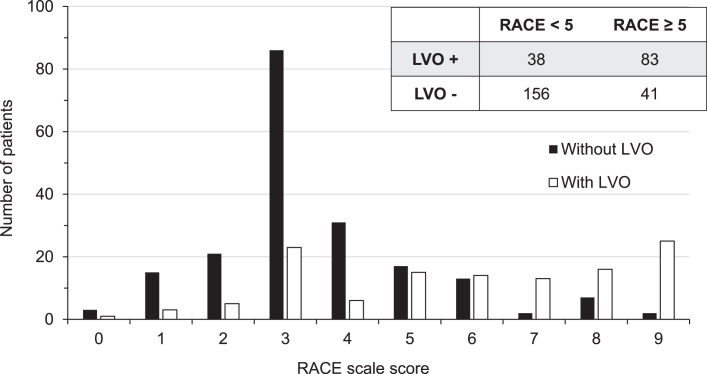
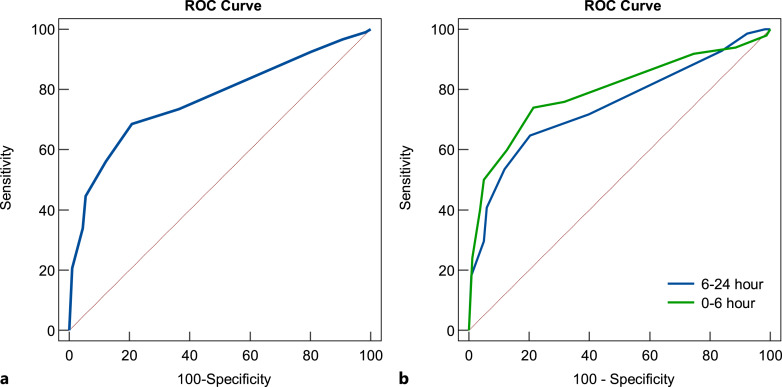
Results: There were 318 patients included. LVO was detected in 121/318 patients (37.6%). The higher the RACE score, the higher the proportion of patients with LVO (p < 0.001). Receiver operating characteristic curves showed capacity to predict LVO of the RACE scale with an area under the curve (AUC) of 0.767. The optimal RACE cutoff was ≥5 with sensitivity = 0.68, specificity = 0.79, positive predictive value = 0.67, negative predictive value = 0.80, and overall accuracy = 0.75. RACE ≥5 had higher sensitivity and same specificity for detecting LVO in AIS patients within 6-h versus 6-24-h window (AUC = 0.79 vs. 0.75, sensitivity = 0.74 vs. 0.65, specificity = 0.79 vs. 0.80, accuracy = 0.77 vs. 0.74).
Conclusions: The RACE scale is a simple tool that can accurately identify AIS patients with LVO. This tool may be useful for early detection of LVO patients and should be validated in the prehospital setting in Vietnam.
期刊介绍:
This open access and online-only journal publishes original articles covering the entire spectrum of stroke and cerebrovascular research, drawing from a variety of specialties such as neurology, internal medicine, surgery, radiology, epidemiology, cardiology, hematology, psychology and rehabilitation. Offering an international forum, it meets the growing need for sophisticated, up-to-date scientific information on clinical data, diagnostic testing, and therapeutic issues. The journal publishes original contributions, reviews of selected topics as well as clinical investigative studies. All aspects related to clinical advances are considered, while purely experimental work appears only if directly relevant to clinical issues. Cerebrovascular Diseases Extra provides additional contents based on reviewed and accepted submissions to the main journal Cerebrovascular Diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
