{"title":"Venetoclax Plus Intensified Chemoimmunotherapy as a Bridge to Allogeneic Stem Cell Transplantation in Richter Syndrome: Report of Two Cases.","authors":"Enrico Derenzini, Alessandro Cignetti, Valentina Tabanelli, Daniela Gottardi, Elvira Gerbino, Anna Vanazzi, Simona Sammassimo, Alessio Maria Edoardo Maraglino, Federica Melle, Giovanna Motta, Daniela Malengo, Emanuela Omodeo Salè, Lisa Bonello, Rocco Pastano, Stefano Pileri, Fabrizio Carnevale Schianca, Corrado Tarella","doi":"10.3390/hematolrep16040075","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Richter syndrome (RS) represents a major unmet need in the lymphoma field, being refractory to chemoimmunotherapy and targeted agents. The BCL-2 inhibitor venetoclax in combination with dose-adjusted EPOCH-R chemoimmunotherapy showed promising efficacy in patients affected by RS. However, responses were not durable, suggesting the need for further treatment optimization. <b>Methods:</b> Here, we report two cases of RS achieving long-term complete remission with intensified chemoimmunotherapy (Rituximab-G-MALL B-ALL/NHL2002 regimen) plus venetoclax induction, followed by haploidentical hematopoietic stem cell transplant (allo-HSCT). Venetoclax was given continuously for 14 consecutive days after every Rituximab-G-MALL cycle in off-label use. An accelerated venetoclax rump-up schedule was used in both patients to reach the maximal dose. Maximal venetoclax dose was 300 mg and 400 mg in patient 1 and patient 2, respectively. <b>Results:</b> The combined treatment was well tolerated, with no major infective complications or non-hematological toxicities. In both patients, immunosuppression was discontinued within day 180 after transplant with no graft-versus-host-disease flares. Both patients are alive and in continuous complete remission after 60 and 72 months following allo-HSCT. <b>Conclusions:</b> This report supports the feasibility of a combination treatment with BCL-2 inhibitors and intensive chemoimmunotherapy as a bridge to allo-HSCT in RS.</p>","PeriodicalId":12829,"journal":{"name":"Hematology Reports","volume":"16 4","pages":"795-803"},"PeriodicalIF":1.2000,"publicationDate":"2024-12-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11728234/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hematology Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/hematolrep16040075","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
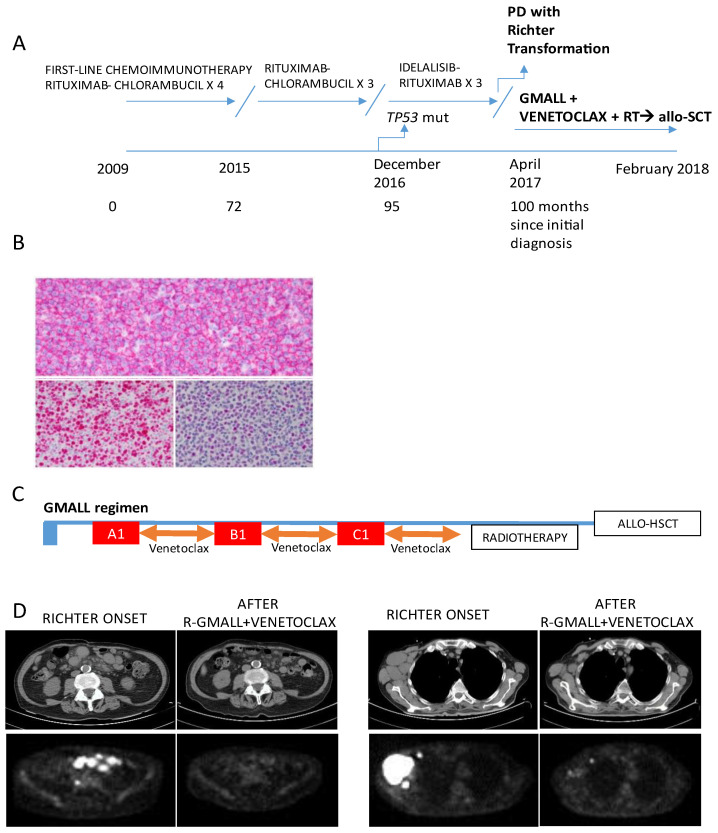
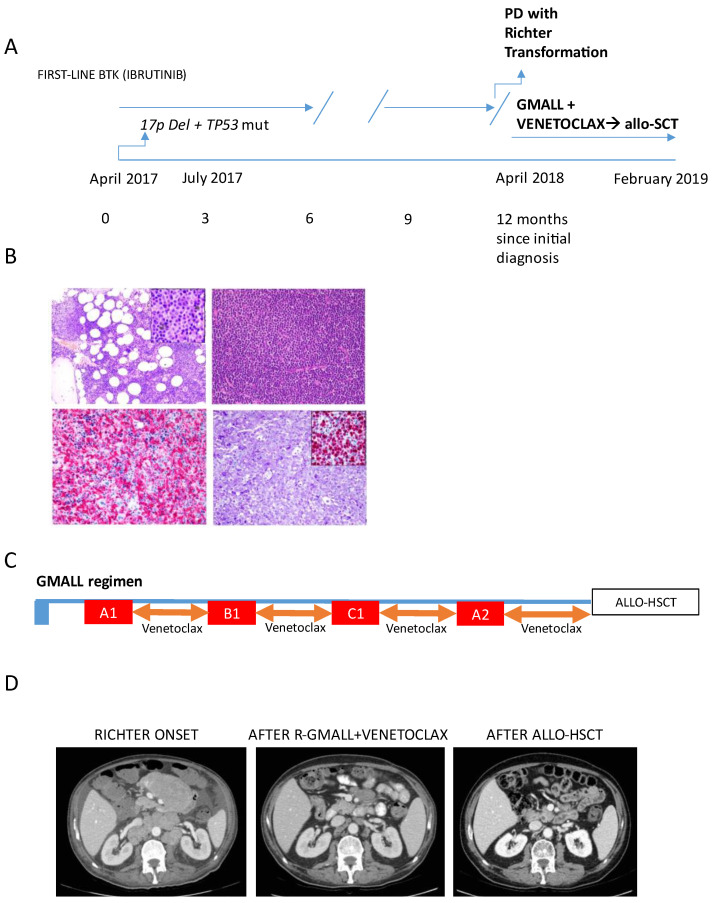
Background: Richter syndrome (RS) represents a major unmet need in the lymphoma field, being refractory to chemoimmunotherapy and targeted agents. The BCL-2 inhibitor venetoclax in combination with dose-adjusted EPOCH-R chemoimmunotherapy showed promising efficacy in patients affected by RS. However, responses were not durable, suggesting the need for further treatment optimization. Methods: Here, we report two cases of RS achieving long-term complete remission with intensified chemoimmunotherapy (Rituximab-G-MALL B-ALL/NHL2002 regimen) plus venetoclax induction, followed by haploidentical hematopoietic stem cell transplant (allo-HSCT). Venetoclax was given continuously for 14 consecutive days after every Rituximab-G-MALL cycle in off-label use. An accelerated venetoclax rump-up schedule was used in both patients to reach the maximal dose. Maximal venetoclax dose was 300 mg and 400 mg in patient 1 and patient 2, respectively. Results: The combined treatment was well tolerated, with no major infective complications or non-hematological toxicities. In both patients, immunosuppression was discontinued within day 180 after transplant with no graft-versus-host-disease flares. Both patients are alive and in continuous complete remission after 60 and 72 months following allo-HSCT. Conclusions: This report supports the feasibility of a combination treatment with BCL-2 inhibitors and intensive chemoimmunotherapy as a bridge to allo-HSCT in RS.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
