Diagnostic Ability of Risk Models in the Field of Ischemic Stroke for Predicting Atherosclerotic Outcomes in Patients with Acute Myocardial Infarction.
{"title":"Diagnostic Ability of Risk Models in the Field of Ischemic Stroke for Predicting Atherosclerotic Outcomes in Patients with Acute Myocardial Infarction.","authors":"Hiroki Goto, Yuichi Saito, Hiroaki Yaginuma, Kazunari Asada, Takanori Sato, Osamu Hashimoto, Hideki Kitahara, Yoshio Kobayashi","doi":"10.5551/jat.65162","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Several risk-scoring models, including the Fukuoka Stroke Risk Score, Essen Stroke Risk Score, and Stroke Prognosis Instrument II, have been developed to predict recurrent cerebrovascular events in patients with ischemic stroke. As myocardial infarction (MI) and ischemic stroke are both atherosclerotic diseases, these scoring models in the field of cerebrovascular disease may be applicable and useful for risk stratification in patients with acute MI. We therefore evaluated the diagnostic ability and clinical applicability of these stroke risk scores in predicting atherosclerotic events after acute MI.</p><p><strong>Methods: </strong>This multicenter retrospective study included 2016 patients with acute MI who underwent percutaneous coronary intervention and survived to discharge. The three risk-scoring models were calculated, and their diagnostic ability for major adverse cardiovascular events (MACE) after discharge, a composite of cardiovascular death, recurrent MI, and ischemic stroke, was evaluated.</p><p><strong>Results: </strong>During the median follow-up of 523 days, 218 (10.8%) patients experienced MACE after discharge. High values for Fukuoka Stroke Risk Score, Essen Stroke Risk Score, and Stroke Prognosis Instrument II were progressively associated with an increased risk of MACE after discharge. Overall, the diagnostic abilities of the three risk scores were similar.</p><p><strong>Conclusions: </strong>Risk prediction models in the field of ischemic stroke, including the Fukuoka Stroke Risk Score, Essen Stroke Risk Score, and Stroke Prognosis Instrument II, were useful in stratifying MACE risk in patients with acute MI. Risk-scoring models for atherosclerotic cardiovascular disease may be applicable to patient populations with other cardiovascular diseases in different arterial territories.</p>","PeriodicalId":15128,"journal":{"name":"Journal of atherosclerosis and thrombosis","volume":" ","pages":"853-862"},"PeriodicalIF":2.8000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12237784/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of atherosclerosis and thrombosis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5551/jat.65162","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/26 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
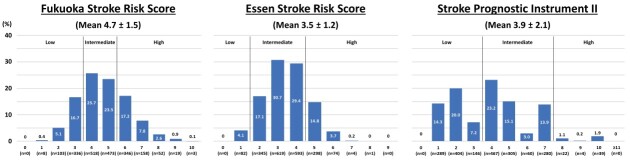
Aims: Several risk-scoring models, including the Fukuoka Stroke Risk Score, Essen Stroke Risk Score, and Stroke Prognosis Instrument II, have been developed to predict recurrent cerebrovascular events in patients with ischemic stroke. As myocardial infarction (MI) and ischemic stroke are both atherosclerotic diseases, these scoring models in the field of cerebrovascular disease may be applicable and useful for risk stratification in patients with acute MI. We therefore evaluated the diagnostic ability and clinical applicability of these stroke risk scores in predicting atherosclerotic events after acute MI.
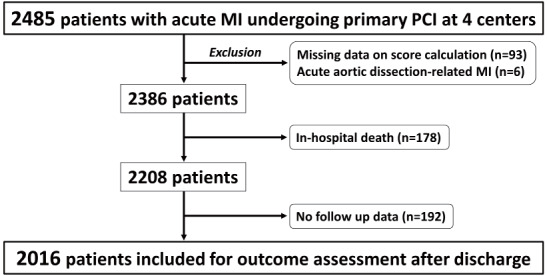
Methods: This multicenter retrospective study included 2016 patients with acute MI who underwent percutaneous coronary intervention and survived to discharge. The three risk-scoring models were calculated, and their diagnostic ability for major adverse cardiovascular events (MACE) after discharge, a composite of cardiovascular death, recurrent MI, and ischemic stroke, was evaluated.
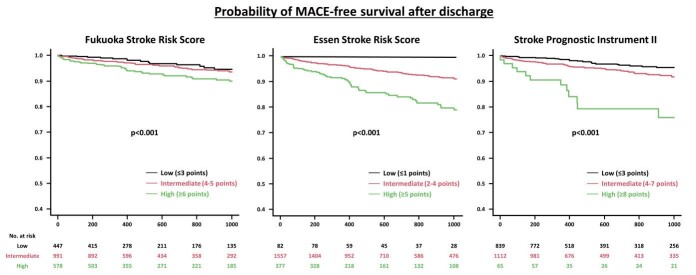
Results: During the median follow-up of 523 days, 218 (10.8%) patients experienced MACE after discharge. High values for Fukuoka Stroke Risk Score, Essen Stroke Risk Score, and Stroke Prognosis Instrument II were progressively associated with an increased risk of MACE after discharge. Overall, the diagnostic abilities of the three risk scores were similar.
Conclusions: Risk prediction models in the field of ischemic stroke, including the Fukuoka Stroke Risk Score, Essen Stroke Risk Score, and Stroke Prognosis Instrument II, were useful in stratifying MACE risk in patients with acute MI. Risk-scoring models for atherosclerotic cardiovascular disease may be applicable to patient populations with other cardiovascular diseases in different arterial territories.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
