{"title":"Nonadjustable state of programmable shunt valve: obstruction of middle cranial fossa arachnoid cyst-peritoneal shunt.","authors":"Hongbin Cao, Genrui Guo, Wenjing Wu, Zhenghai Cheng","doi":"10.1186/s41016-024-00386-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A nonadjustable state of the programmable shunt valve is a rare phenomenon. This case report aims to explore the cause of pressure adjustment dysfunction in a programmable shunt valve in a middle cranial fossa arachnoid cyst-peritoneal shunt patient and to underscore this dysfunction as an indicator of shunt valve obstruction.</p><p><strong>Case presentation: </strong>A child with a ruptured giant arachnoid cyst in the left middle cranial fossa presented with acute intracranial hypertension following head trauma. The initial cysto-peritoneal shunt surgery rapidly alleviated symptoms, including headaches, vomiting, and left cranial nerve palsy, stabilizing the clinical condition. However, between 20 and 24 months after the initial shunt surgery, the patient developed intermittent shunt dysfunction, experiencing recurrent headaches and vomiting, during which the programmable valve's pressure setting had become fixed and was no longer adjustable. A second surgery was then performed to remove the existing shunt, excise the fibrotic cyst wall, fenestrate the basal cistern, and establish temporary subdural drainage. During this operation, extensive fibrosis of the cyst wall in the subdural space was discovered, forming a tough and hypertrophic fibrotic membrane that encased the cerebral hemispheres. This fibrotic material nearly filled the shunt valve chamber, causing valve obstruction and immobilizing the pressure control rod, resulting in pressure adjustment dysfunction. As the patient could not maintain stability without continuous drainage, a third surgery was ultimately necessary to place a subdural-peritoneal shunt. Five years of follow-up revealed no significant clinical symptoms, and the patient has maintained a normal life.</p><p><strong>Conclusion: </strong>Shunt valve obstruction is an underestimated cause of shunt system failure, with no current definitive method for early diagnosis. Fibrotic deposition is a primary mechanism underlying shunt valve obstruction. Pressure adjustment dysfunction in a programmable shunt valve serves as a reliable indicator of shunt valve obstruction. Further research should prioritize the treatment and prevention of shunt valve obstructions to improve outcomes in neurosurgical practice.</p>","PeriodicalId":36700,"journal":{"name":"Chinese Neurosurgical Journal","volume":"10 1","pages":"34"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11670491/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chinese Neurosurgical Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s41016-024-00386-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A nonadjustable state of the programmable shunt valve is a rare phenomenon. This case report aims to explore the cause of pressure adjustment dysfunction in a programmable shunt valve in a middle cranial fossa arachnoid cyst-peritoneal shunt patient and to underscore this dysfunction as an indicator of shunt valve obstruction.
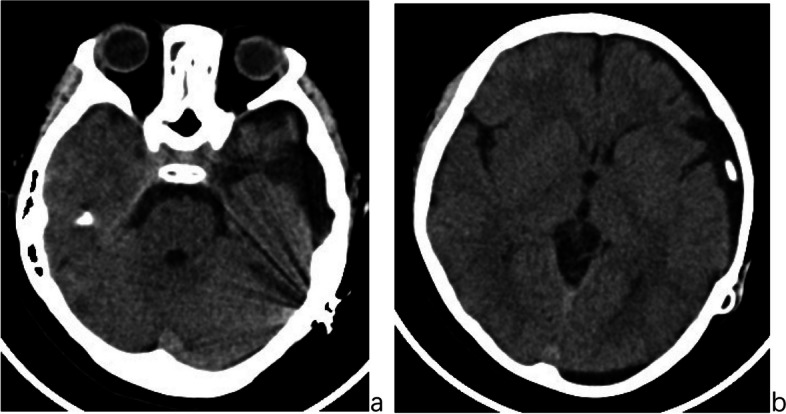
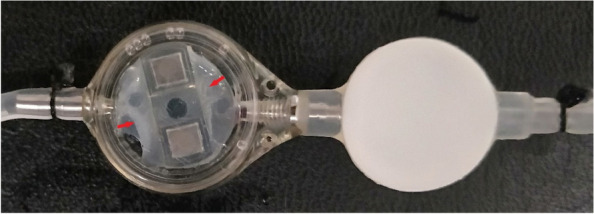
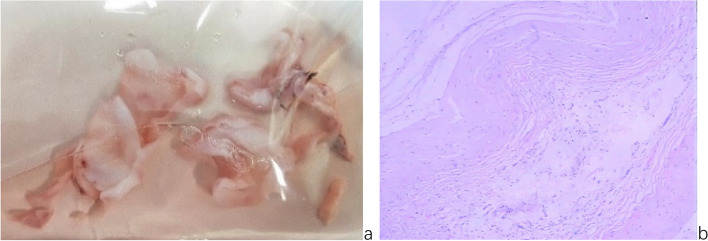
Case presentation: A child with a ruptured giant arachnoid cyst in the left middle cranial fossa presented with acute intracranial hypertension following head trauma. The initial cysto-peritoneal shunt surgery rapidly alleviated symptoms, including headaches, vomiting, and left cranial nerve palsy, stabilizing the clinical condition. However, between 20 and 24 months after the initial shunt surgery, the patient developed intermittent shunt dysfunction, experiencing recurrent headaches and vomiting, during which the programmable valve's pressure setting had become fixed and was no longer adjustable. A second surgery was then performed to remove the existing shunt, excise the fibrotic cyst wall, fenestrate the basal cistern, and establish temporary subdural drainage. During this operation, extensive fibrosis of the cyst wall in the subdural space was discovered, forming a tough and hypertrophic fibrotic membrane that encased the cerebral hemispheres. This fibrotic material nearly filled the shunt valve chamber, causing valve obstruction and immobilizing the pressure control rod, resulting in pressure adjustment dysfunction. As the patient could not maintain stability without continuous drainage, a third surgery was ultimately necessary to place a subdural-peritoneal shunt. Five years of follow-up revealed no significant clinical symptoms, and the patient has maintained a normal life.
Conclusion: Shunt valve obstruction is an underestimated cause of shunt system failure, with no current definitive method for early diagnosis. Fibrotic deposition is a primary mechanism underlying shunt valve obstruction. Pressure adjustment dysfunction in a programmable shunt valve serves as a reliable indicator of shunt valve obstruction. Further research should prioritize the treatment and prevention of shunt valve obstructions to improve outcomes in neurosurgical practice.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
