Impact of pulmonary vein isolation on atrial arrhythmias in patients with typical atrial flutter: systematic review and meta-analysis of randomized clinical trials.
Daniel A Gomes, Rita Reis Santos, Jorge Ferreira, Frédéric Anselme, Peter Calvert, Amand Floriaan Schmidt, Dhiraj Gupta, Serge Boveda, Pedro Adragão, Rui Providência
{"title":"Impact of pulmonary vein isolation on atrial arrhythmias in patients with typical atrial flutter: systematic review and meta-analysis of randomized clinical trials.","authors":"Daniel A Gomes, Rita Reis Santos, Jorge Ferreira, Frédéric Anselme, Peter Calvert, Amand Floriaan Schmidt, Dhiraj Gupta, Serge Boveda, Pedro Adragão, Rui Providência","doi":"10.1093/ehjopen/oeae102","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Cavotricuspid isthmus (CTI) ablation is the current ablation treatment for typical atrial flutter (AFL). However, post-ablation atrial tachyarrhythmias, mostly in the form of atrial fibrillation (AF), are frequently observed after CTI ablation. We aimed to evaluate the effectiveness and safety of concomitant or isolated pulmonary vein isolation (PVI) in patients with typical AFL scheduled for ablation.</p><p><strong>Methods and results: </strong>Electronic databases (PubMED, EMBASE, Clinicaltrials.gov) were searched through July, 2024. Randomized controlled trials (RCTs) were eligible if comparing PVI ± CTI ablation vs. CTI alone. The primary outcomes were any sustained atrial arrhythmia, typical AFL relapse, and AF. Secondary outcomes were need for redo-ablation or antiarrhythmic drugs. Random-effects and fixed-effects meta-analyses were undertaken for each individual outcome. Seven RCTs, with a total of 902 patients, were included. Comparing to CTI ablation alone, PVI ± CTI was more effective in preventing atrial tachyarrhythmias [risk ratio (RR) = 0.57, 95% CI: 0.41-0.79, <i>P</i> = 0.0007, <i>I</i> <sup>2</sup> = 50%, number needed to treat (NNT) = 4.1]. The results were driven mainly by a reduction of new onset/recurrent AF (RR = 0.41, 95% CI: 0.27-0.61, <i>P</i> < 0.0001, <i>I</i> <sup>2</sup> = 0%, NNT = 3.3), whereas there were no differences in typical AFL relapse (RR = 1.52, 95% CI: 0.63-3.66, <i>P</i> = 0.35, <i>I</i> <sup>2</sup> = 9%). Major complication rate was low and comparable across groups, although uncomplicated pericardial effusion was higher in PVI ± CTI (1.8% vs. 0.0%, <i>P</i> = 0.04). Results were comparable for the sub-analysis of PVI alone vs. CTI ablation.</p><p><strong>Conclusion: </strong>In patients with typical AFL, PVI ± CTI ablation is more effective than CTI alone in reducing the atrial tachyarrhythmias and subsequent AF during follow-up, without affecting major complications rate. These results set the rationale for a well-designed, larger-scale RCT comparing both strategies.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 1","pages":"oeae102"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11668177/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeae102","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
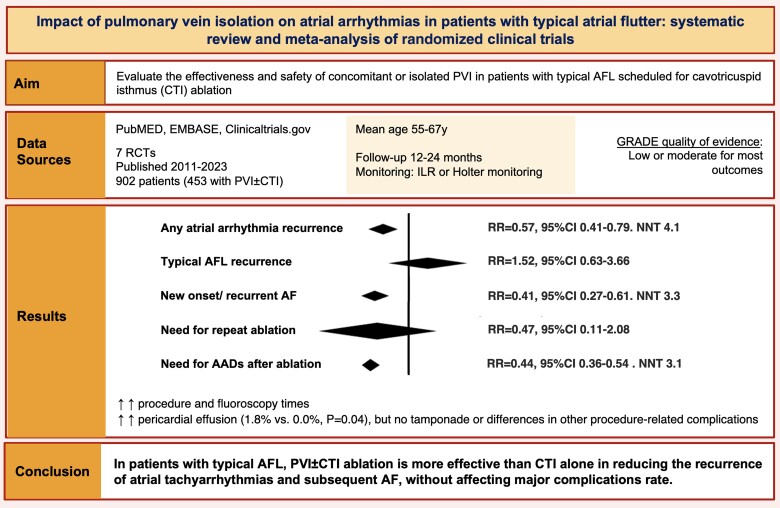
Aims: Cavotricuspid isthmus (CTI) ablation is the current ablation treatment for typical atrial flutter (AFL). However, post-ablation atrial tachyarrhythmias, mostly in the form of atrial fibrillation (AF), are frequently observed after CTI ablation. We aimed to evaluate the effectiveness and safety of concomitant or isolated pulmonary vein isolation (PVI) in patients with typical AFL scheduled for ablation.
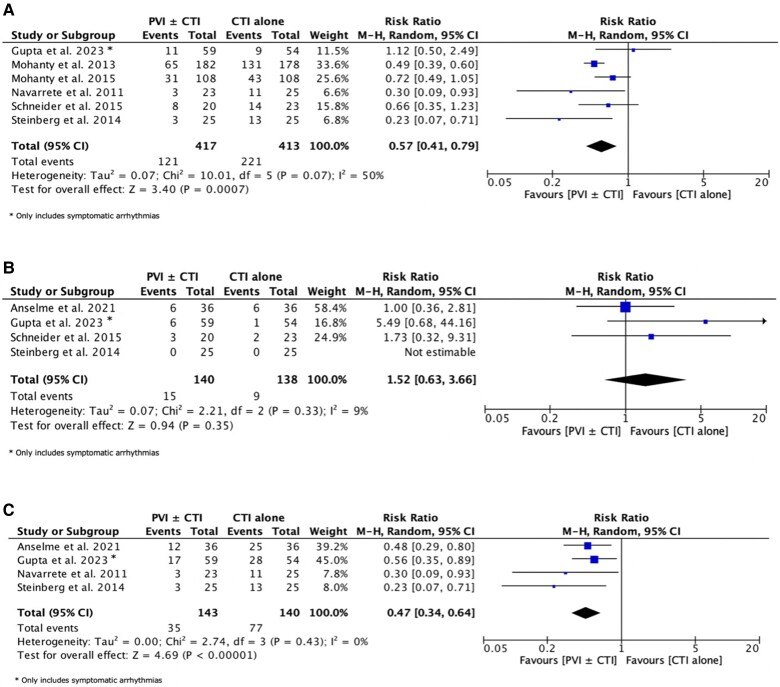
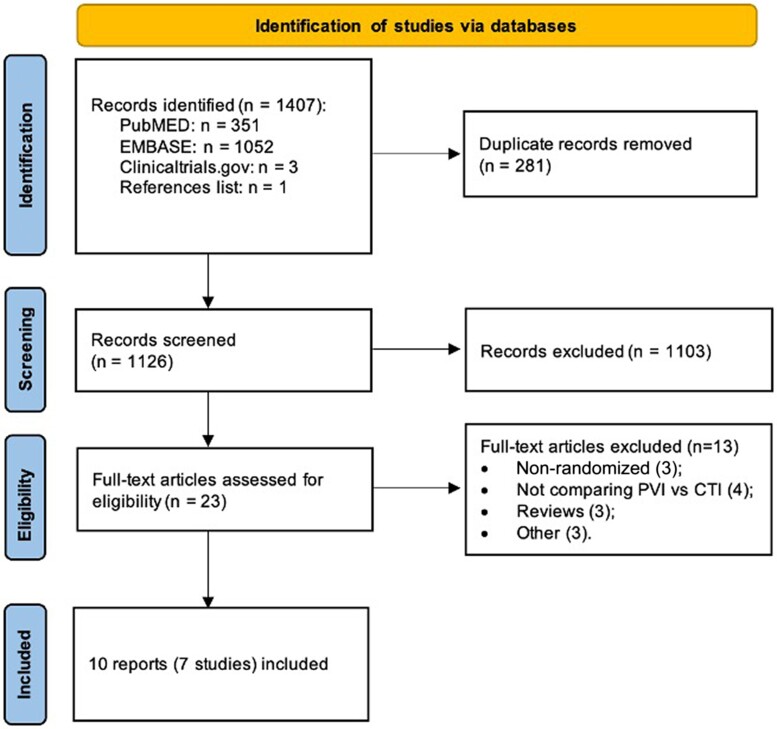
Methods and results: Electronic databases (PubMED, EMBASE, Clinicaltrials.gov) were searched through July, 2024. Randomized controlled trials (RCTs) were eligible if comparing PVI ± CTI ablation vs. CTI alone. The primary outcomes were any sustained atrial arrhythmia, typical AFL relapse, and AF. Secondary outcomes were need for redo-ablation or antiarrhythmic drugs. Random-effects and fixed-effects meta-analyses were undertaken for each individual outcome. Seven RCTs, with a total of 902 patients, were included. Comparing to CTI ablation alone, PVI ± CTI was more effective in preventing atrial tachyarrhythmias [risk ratio (RR) = 0.57, 95% CI: 0.41-0.79, P = 0.0007, I2 = 50%, number needed to treat (NNT) = 4.1]. The results were driven mainly by a reduction of new onset/recurrent AF (RR = 0.41, 95% CI: 0.27-0.61, P < 0.0001, I2 = 0%, NNT = 3.3), whereas there were no differences in typical AFL relapse (RR = 1.52, 95% CI: 0.63-3.66, P = 0.35, I2 = 9%). Major complication rate was low and comparable across groups, although uncomplicated pericardial effusion was higher in PVI ± CTI (1.8% vs. 0.0%, P = 0.04). Results were comparable for the sub-analysis of PVI alone vs. CTI ablation.
Conclusion: In patients with typical AFL, PVI ± CTI ablation is more effective than CTI alone in reducing the atrial tachyarrhythmias and subsequent AF during follow-up, without affecting major complications rate. These results set the rationale for a well-designed, larger-scale RCT comparing both strategies.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
