Rebecca M Glendell, Kathryn A Puxty, Martin Shaw, Malcolm Ab Sim, Jamie P Traynor, Patrick B Mark, Mark Andonovic
{"title":"Longitudinal trend in post-discharge estimated glomerular filtration rate in intensive care survivors.","authors":"Rebecca M Glendell, Kathryn A Puxty, Martin Shaw, Malcolm Ab Sim, Jamie P Traynor, Patrick B Mark, Mark Andonovic","doi":"10.1177/17511437241308673","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute kidney injury (AKI) within the intensive care unit (ICU) is common but evidence is limited on longer-term renal outcomes. We aimed to model the trend of kidney function in ICU survivors using estimated glomerular filtration rate (eGFR), comparing those with and without AKI, and investigate potential risk factors associated with eGFR decline.</p><p><strong>Methods: </strong>This observational cohort study included all patients aged 16 or older admitted to two general adult ICUs in Scotland between 1st July 2015 and 30th June 2018 who survived to 30 days following hospital discharge. Baseline serum creatinine and subsequent values were used to identify patients with AKI and calculate eGFR following hospital discharge. Mixed effects modelling was used to control for repeated measures and to allow inclusion of several exploratory variables.</p><p><strong>Results: </strong>3649 patients were included, with 1252 (34%) experiencing in-ICU AKI. Patients were followed up for up to 2000 days with a median 21 eGFR measurements. eGFR declined at a rate of -1.9 ml/min/1.73m<sup>2</sup>/year (<i>p-</i>value < 0.001) in the overall ICU survivor cohort. Patients with AKI experienced an accelerated rate of post-ICU eGFR decline of -2.0 ml/min/1.73m<sup>2</sup>/year compared to a rate of -1.83 ml/min/1.73m<sup>2</sup>/year in patients who did not experience AKI (<i>p-</i>value 0.007). Pre-existing diabetes or liver disease and in-ICU vasopressor support were associated with accelerated eGFR decline regardless of AKI experience.</p><p><strong>Conclusions: </strong>ICU survivors experienced a decline in kidney function beyond that which would be expected regardless of in-ICU AKI. Long-term follow-up is warranted in ICU survivors to monitor kidney function and reduce morbidity and mortality.</p>","PeriodicalId":39161,"journal":{"name":"Journal of the Intensive Care Society","volume":" ","pages":"29-37"},"PeriodicalIF":1.4000,"publicationDate":"2024-12-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11670225/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Intensive Care Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/17511437241308673","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Acute kidney injury (AKI) within the intensive care unit (ICU) is common but evidence is limited on longer-term renal outcomes. We aimed to model the trend of kidney function in ICU survivors using estimated glomerular filtration rate (eGFR), comparing those with and without AKI, and investigate potential risk factors associated with eGFR decline.
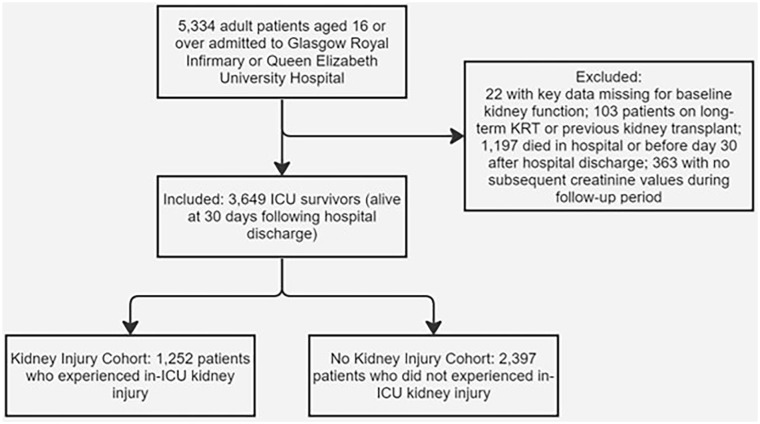
Methods: This observational cohort study included all patients aged 16 or older admitted to two general adult ICUs in Scotland between 1st July 2015 and 30th June 2018 who survived to 30 days following hospital discharge. Baseline serum creatinine and subsequent values were used to identify patients with AKI and calculate eGFR following hospital discharge. Mixed effects modelling was used to control for repeated measures and to allow inclusion of several exploratory variables.
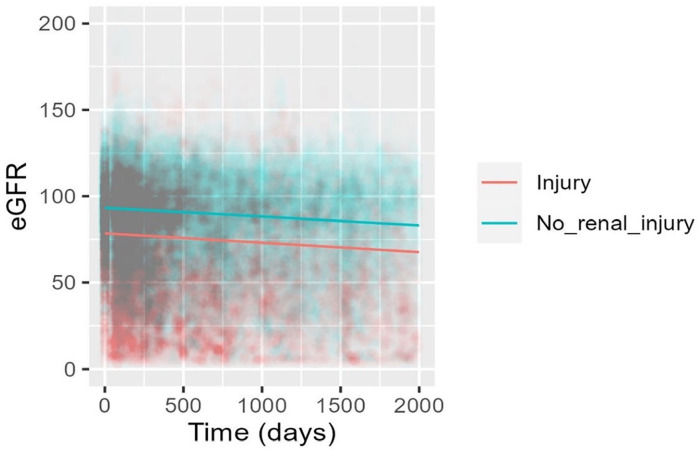
Results: 3649 patients were included, with 1252 (34%) experiencing in-ICU AKI. Patients were followed up for up to 2000 days with a median 21 eGFR measurements. eGFR declined at a rate of -1.9 ml/min/1.73m2/year (p-value < 0.001) in the overall ICU survivor cohort. Patients with AKI experienced an accelerated rate of post-ICU eGFR decline of -2.0 ml/min/1.73m2/year compared to a rate of -1.83 ml/min/1.73m2/year in patients who did not experience AKI (p-value 0.007). Pre-existing diabetes or liver disease and in-ICU vasopressor support were associated with accelerated eGFR decline regardless of AKI experience.
Conclusions: ICU survivors experienced a decline in kidney function beyond that which would be expected regardless of in-ICU AKI. Long-term follow-up is warranted in ICU survivors to monitor kidney function and reduce morbidity and mortality.
期刊介绍:
The Journal of the Intensive Care Society (JICS) is an international, peer-reviewed journal that strives to disseminate clinically and scientifically relevant peer-reviewed research, evaluation, experience and opinion to all staff working in the field of intensive care medicine. Our aim is to inform clinicians on the provision of best practice and provide direction for innovative scientific research in what is one of the broadest and most multi-disciplinary healthcare specialties. While original articles and systematic reviews lie at the heart of the Journal, we also value and recognise the need for opinion articles, case reports and correspondence to guide clinically and scientifically important areas in which conclusive evidence is lacking. The style of the Journal is based on its founding mission statement to ‘instruct, inform and entertain by encompassing the best aspects of both tabloid and broadsheet''.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
