Johan Ahti, Tuula Kieseppä, Willehard Haaki, Jaana Suvisaari, Solja Niemelä, Kimmo Suokas, Minna Holm, Asko Wegelius, Olli Kampman, Markku Lähteenvuo, Tiina Paunio, Jari Tiihonen, Jarmo Hietala, Erkki Isometsä
{"title":"General medical comorbidities in psychotic disorders in the Finnish SUPER study.","authors":"Johan Ahti, Tuula Kieseppä, Willehard Haaki, Jaana Suvisaari, Solja Niemelä, Kimmo Suokas, Minna Holm, Asko Wegelius, Olli Kampman, Markku Lähteenvuo, Tiina Paunio, Jari Tiihonen, Jarmo Hietala, Erkki Isometsä","doi":"10.1038/s41537-024-00546-1","DOIUrl":null,"url":null,"abstract":"<p><p>Schizophrenia (SZ), schizoaffective disorder (SZA), bipolar disorder (BD), and psychotic depression (PD) are associated with premature death due to preventable general medical comorbidities (GMCs). The interaction between psychosis, risk factors, and GMCs is complex and should be elucidated. More research particularly among those with SZA or PD is warranted. We evaluated the association between registry-based psychotic disorders and GMC diagnoses in a large national sample of participants with different psychotic disorders. In addition, we examined whether body mass index (BMI) and smoking as risk factors for GMCs explain differences between diagnostic groups. This was a cross-sectional study of a clinical population of participants (n = 10,417) in the Finnish SUPER study. Registry-based diagnoses of psychotic disorders and hypertension, diabetes, chronic obstructive pulmonary disease (COPD), cancers, ischemic heart disease, and liver disorders were obtained. Participants' BMI and self-reported smoking were recorded. Total effect of diagnostic category adjusted for age and sex as well as direct effect including known risk factors was calculated using logistic regression. Regardless of diagnostic category, participants had high BMI (average 30.3 kg/m<sup>2</sup>), and current smoking was common (42.4%). Diabetes and COPD were more common in SZ than in other diagnostic categories. The differences between psychotic disorders were not explained by obesity or smoking status only. Obesity and smoking were prevalent in all diagnostic categories of psychotic disorders, and continued efforts at prevention are warranted. Additional differences in GMC prevalence exist between psychotic disorders that are not explained by obesity and smoking.</p>","PeriodicalId":74758,"journal":{"name":"Schizophrenia (Heidelberg, Germany)","volume":"10 1","pages":"124"},"PeriodicalIF":4.1000,"publicationDate":"2024-12-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11688420/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Schizophrenia (Heidelberg, Germany)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1038/s41537-024-00546-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
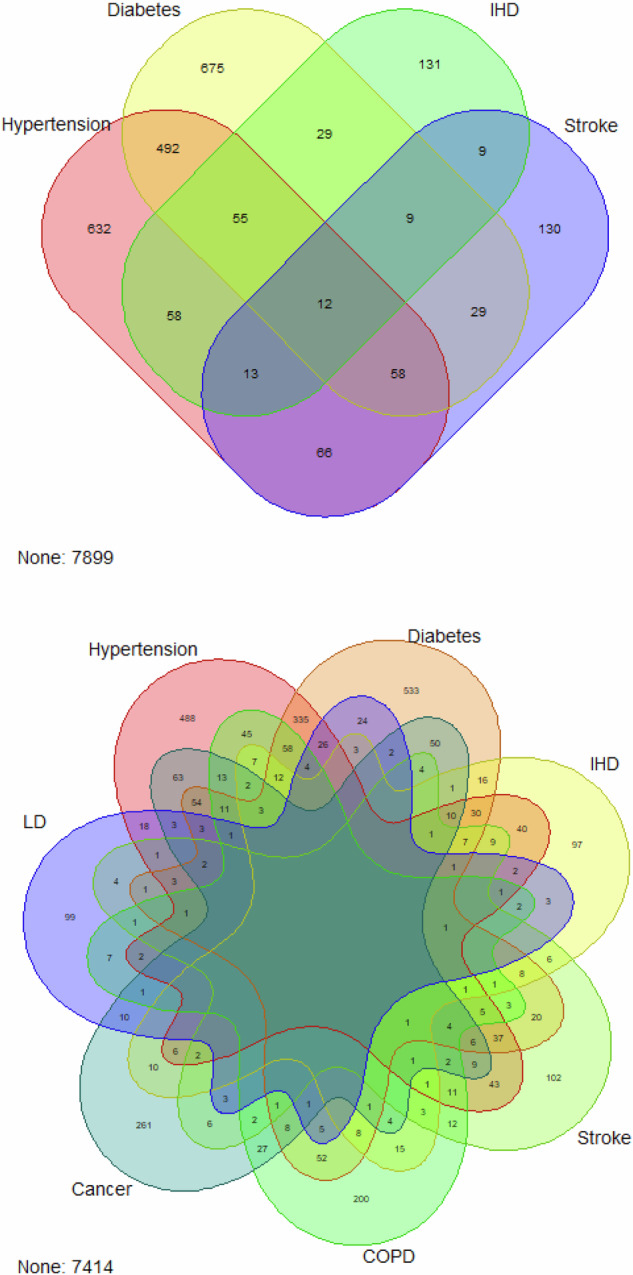
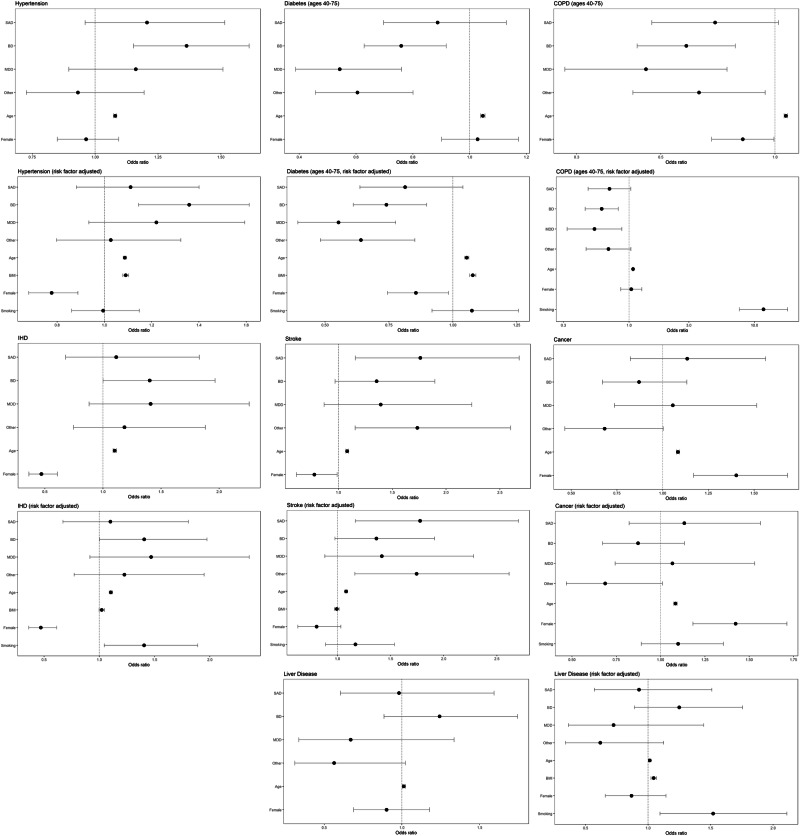
Schizophrenia (SZ), schizoaffective disorder (SZA), bipolar disorder (BD), and psychotic depression (PD) are associated with premature death due to preventable general medical comorbidities (GMCs). The interaction between psychosis, risk factors, and GMCs is complex and should be elucidated. More research particularly among those with SZA or PD is warranted. We evaluated the association between registry-based psychotic disorders and GMC diagnoses in a large national sample of participants with different psychotic disorders. In addition, we examined whether body mass index (BMI) and smoking as risk factors for GMCs explain differences between diagnostic groups. This was a cross-sectional study of a clinical population of participants (n = 10,417) in the Finnish SUPER study. Registry-based diagnoses of psychotic disorders and hypertension, diabetes, chronic obstructive pulmonary disease (COPD), cancers, ischemic heart disease, and liver disorders were obtained. Participants' BMI and self-reported smoking were recorded. Total effect of diagnostic category adjusted for age and sex as well as direct effect including known risk factors was calculated using logistic regression. Regardless of diagnostic category, participants had high BMI (average 30.3 kg/m2), and current smoking was common (42.4%). Diabetes and COPD were more common in SZ than in other diagnostic categories. The differences between psychotic disorders were not explained by obesity or smoking status only. Obesity and smoking were prevalent in all diagnostic categories of psychotic disorders, and continued efforts at prevention are warranted. Additional differences in GMC prevalence exist between psychotic disorders that are not explained by obesity and smoking.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
