{"title":"A rare case of Gardnerella vaginalis spondylodiscitis","authors":"Alex Belote, Kassem Hammoud","doi":"10.1016/j.idcr.2024.e02126","DOIUrl":null,"url":null,"abstract":"<div><div>A 55-year-old-male with a chronic left uretero-pelvic junction (UPJ) obstruction managed with intermittent stent exchanges presented with low midline back pain. CT Abdomen/Pelvis revealed spondylodiscitis at L4-L5, further demonstrated on MRI Lumbar spine. Imaging also revealed the left nephro-ureteral stent was mispositioned, with some mild wall thickening of the left ureter. He was not systemically ill, and antimicrobials were held. He underwent a L4/5 disc biopsy, and pathology revealed acute discitis. Blood and biopsy cultures remained negative through hospital day 5. He then underwent repeat L4/5 disc biopsy. Cultures of repeat biopsy resulted in <em>Gardnerella vaginalis</em>. IV antimicrobials were stopped, and oral Metronidazole was started. He completed 10 weeks of Metronidazole therapy, with significant clinical improvement.</div><div><em>G. vaginalis</em> is a rare cause of bone and joint infections. It is difficult to culture and is less virulent than common bacteria associated with native vertebral osteomyelitis. There have been few case reports of <em>G. vaginalis</em> osteomyelitis or prosthetic joint infection, especially in males. <em>G. vaginalis</em> can rarely colonize the urethra in men and has been known to form biofilm on foreign material in the female genitourinary system. We suspect our patient had developed colonization of his ureteral stent, predisposing him to osteomyelitis. Were repeat biopsy not pursued in this case, our patient likely could have developed empiric treatment failure. Holding antibiotics after initial biopsy proved highly beneficial.</div></div>","PeriodicalId":47045,"journal":{"name":"IDCases","volume":"39 ","pages":"Article e02126"},"PeriodicalIF":1.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11699804/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"IDCases","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2214250924002026","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/12 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
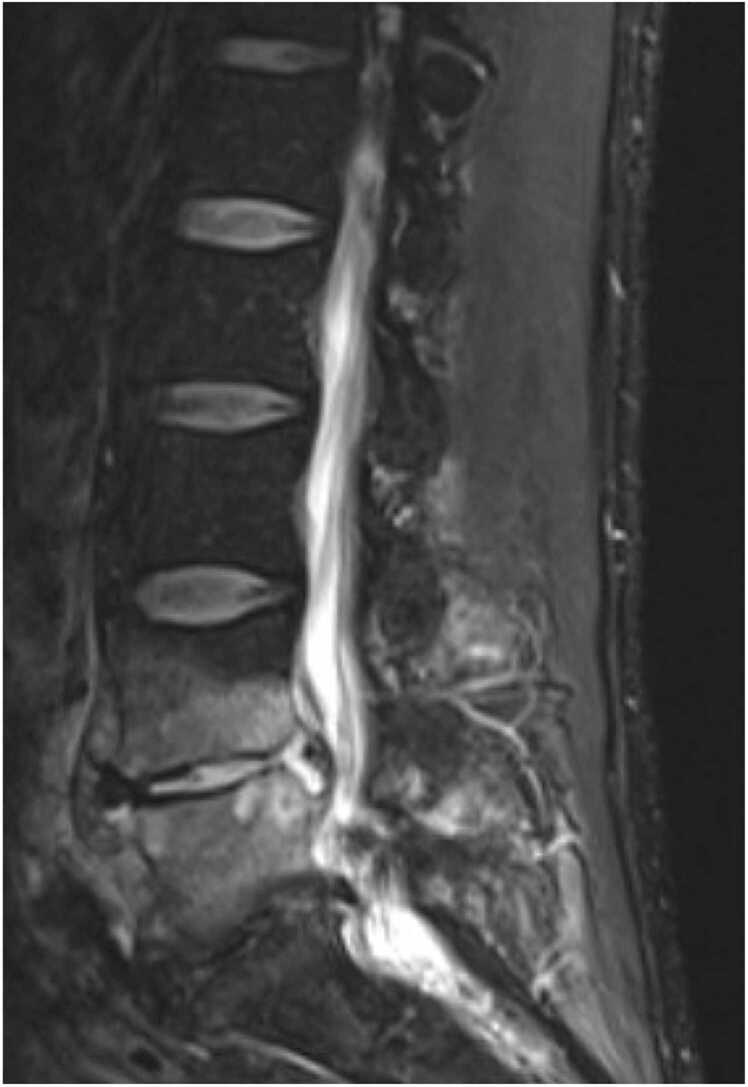
A 55-year-old-male with a chronic left uretero-pelvic junction (UPJ) obstruction managed with intermittent stent exchanges presented with low midline back pain. CT Abdomen/Pelvis revealed spondylodiscitis at L4-L5, further demonstrated on MRI Lumbar spine. Imaging also revealed the left nephro-ureteral stent was mispositioned, with some mild wall thickening of the left ureter. He was not systemically ill, and antimicrobials were held. He underwent a L4/5 disc biopsy, and pathology revealed acute discitis. Blood and biopsy cultures remained negative through hospital day 5. He then underwent repeat L4/5 disc biopsy. Cultures of repeat biopsy resulted in Gardnerella vaginalis. IV antimicrobials were stopped, and oral Metronidazole was started. He completed 10 weeks of Metronidazole therapy, with significant clinical improvement.
G. vaginalis is a rare cause of bone and joint infections. It is difficult to culture and is less virulent than common bacteria associated with native vertebral osteomyelitis. There have been few case reports of G. vaginalis osteomyelitis or prosthetic joint infection, especially in males. G. vaginalis can rarely colonize the urethra in men and has been known to form biofilm on foreign material in the female genitourinary system. We suspect our patient had developed colonization of his ureteral stent, predisposing him to osteomyelitis. Were repeat biopsy not pursued in this case, our patient likely could have developed empiric treatment failure. Holding antibiotics after initial biopsy proved highly beneficial.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
