{"title":"Remnant Stomach Influx Reduces Esophageal Reflux and Malnutrition After Proximal Gastrectomy With Double Tract Reconstruction.","authors":"Ryohei Nishiguchi, Takeshi Shimakawa, Shinichi Asaka, Masako Ogawa, Kentaro Yamaguchi, Minoru Murayama, Masano Sagawa, Kotaro Kuhara, Takebumi Usui, Hajime Yokomizo, Shunichi Shiozawa","doi":"10.21873/cdp.10413","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>Remnant stomach influx (RSI) from the anastomotic jejunal-remnant stomach, a physiological food passage, develops after proximal gastrectomy with double-tract reconstruction (PGDT). Sometimes, food passes into the jejunal-loop (JL). We investigated the association of the food passage route in PGDT (RSI/JL) with postoperative esophageal reflux and malnutrition.</p><p><strong>Patients and methods: </strong>We retrospectively collected data for 50 patients with upper-third gastric cancer and esophagogastric junction cancer with PGDT. Using one-year postoperative fluoroscopy findings, 40 propensity score-matched patients were classified into RSI and JL groups (n=20/group), respectively. The groups were comparatively evaluated for: clinicopathological characteristics [age, sex, body mass index (BMI), visceral fat index (VFI), subcutaneous fat index (SFI), skeletal muscle index, pathological stage]; perioperative factors [approach, postoperative complications ≥ Clavien-Dindo Grade 2, postoperative food passage); and esophageal reflux (reflux esophagitis frequency ≥ Grade A, degree of reflux based on fluoroscopy findings). Univariate and multivariate analysis identified predictive factors for post-operative malnutrition in all 50 patients.</p><p><strong>Results: </strong>After propensity score matching, grade of reflux esophagitis and degree of reflux was significantly lower (p=0.014, p<0.001) in the RSI versus JL group. The RSI group showed significantly attenuated percent decrease in BMI, VFI, and SFI (p=0.049, p=0.002, p=0.006). Multivariate analysis identified food passage route (JL) and pathological stage as predictive factors for postoperative malnutrition.</p><p><strong>Conclusion: </strong>Postoperative esophageal reflux and malnutrition were attenuated by food passage mainly via the RSI after PGDT. Improved jejunal-remnant stomach is requisite to ensure satisfactory remnant stomach influx.</p>","PeriodicalId":72510,"journal":{"name":"Cancer diagnosis & prognosis","volume":"5 1","pages":"62-71"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11696333/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer diagnosis & prognosis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21873/cdp.10413","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background/aim: Remnant stomach influx (RSI) from the anastomotic jejunal-remnant stomach, a physiological food passage, develops after proximal gastrectomy with double-tract reconstruction (PGDT). Sometimes, food passes into the jejunal-loop (JL). We investigated the association of the food passage route in PGDT (RSI/JL) with postoperative esophageal reflux and malnutrition.
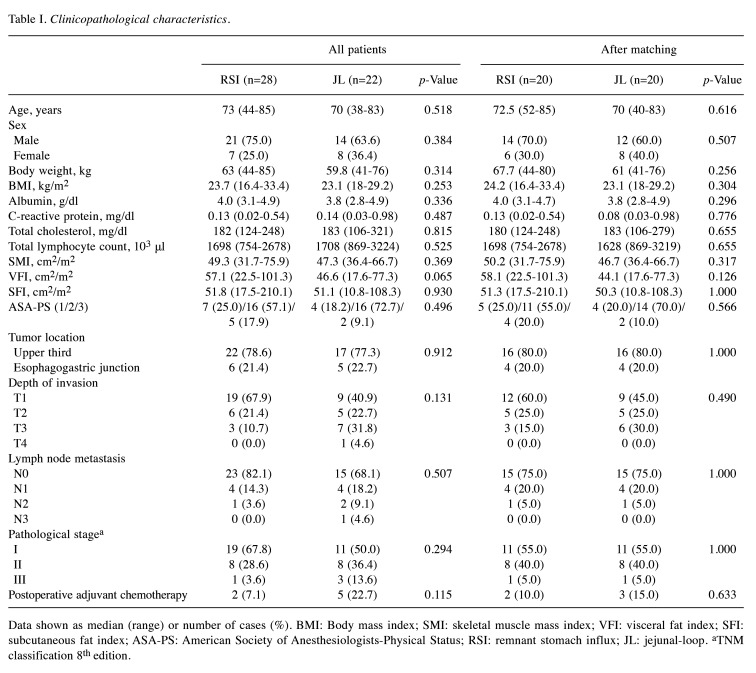
Patients and methods: We retrospectively collected data for 50 patients with upper-third gastric cancer and esophagogastric junction cancer with PGDT. Using one-year postoperative fluoroscopy findings, 40 propensity score-matched patients were classified into RSI and JL groups (n=20/group), respectively. The groups were comparatively evaluated for: clinicopathological characteristics [age, sex, body mass index (BMI), visceral fat index (VFI), subcutaneous fat index (SFI), skeletal muscle index, pathological stage]; perioperative factors [approach, postoperative complications ≥ Clavien-Dindo Grade 2, postoperative food passage); and esophageal reflux (reflux esophagitis frequency ≥ Grade A, degree of reflux based on fluoroscopy findings). Univariate and multivariate analysis identified predictive factors for post-operative malnutrition in all 50 patients.
Results: After propensity score matching, grade of reflux esophagitis and degree of reflux was significantly lower (p=0.014, p<0.001) in the RSI versus JL group. The RSI group showed significantly attenuated percent decrease in BMI, VFI, and SFI (p=0.049, p=0.002, p=0.006). Multivariate analysis identified food passage route (JL) and pathological stage as predictive factors for postoperative malnutrition.
Conclusion: Postoperative esophageal reflux and malnutrition were attenuated by food passage mainly via the RSI after PGDT. Improved jejunal-remnant stomach is requisite to ensure satisfactory remnant stomach influx.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
