{"title":"Predicting In-Hospital Mortality in Patients with End-Stage Renal Disease Receiving Extracorporeal Membrane Oxygenation Therapy.","authors":"Tsung-Yu Tsai, Pei-Chun Fan, Cheng-Chia Lee, Shao-Wei Chen, Jia-Jin Chen, Ming-Jen Chan, Ji-Tseng Fang, Yung-Chang Chen, Chih-Hsiang Chang","doi":"10.1159/000543434","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Patients on extracorporeal membrane oxygenation (ECMO) often experience worse renal outcomes and higher mortality rates as the severity of kidney injury increases. Nevertheless, the in-hospital mortality risks of patients with end-stage renal disease (ESRD) are poorly understood. This study evaluated several prognostic factors associated with in-hospital mortality in patients with ESRD receiving ECMO therapy.</p><p><strong>Methods: </strong>This study reviewed the medical records of 90 adult patients with ESRD on venoarterial ECMO in intensive care units in Linkou Chang Gung Memorial Hospital between March 2009 and February 2022. Fourteen patients who died within 24 h of receiving ECMO support were excluded; the remaining 76 patients were enrolled. Demographic, clinical, and laboratory variables were retrospectively collected as survival predictors. The primary outcome was in-hospital mortality.</p><p><strong>Results: </strong>The overall in-hospital mortality rate was 69.7%. The most common diagnosis requiring ECMO support was postcardiotomy cardiogenic shock, and the most frequent ECMO-associated complication was infection. Multiple logistic regression analysis revealed that the Acute Physiology and Chronic Health Evaluation II (APACHE II) score on day 1 of ECMO support was an independent risk factor for in-hospital mortality. The APACHE II score demonstrated satisfactory discriminative power (0.788 ± 0.057) in the area under the receiver operating characteristic curve. The cumulative survival rates at the 6-month follow-up differed significantly (p < 0.001) between patients with APACHE II score ≤ 29 versus those with APACHE II score >29.</p><p><strong>Conclusion: </strong>For patients with ESRD on ECMO, the APACHE II score is an excellent predictor of in-hospital mortality.</p>","PeriodicalId":9584,"journal":{"name":"Cardiorenal Medicine","volume":" ","pages":"164-173"},"PeriodicalIF":2.9000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11844689/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiorenal Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000543434","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/8 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Patients on extracorporeal membrane oxygenation (ECMO) often experience worse renal outcomes and higher mortality rates as the severity of kidney injury increases. Nevertheless, the in-hospital mortality risks of patients with end-stage renal disease (ESRD) are poorly understood. This study evaluated several prognostic factors associated with in-hospital mortality in patients with ESRD receiving ECMO therapy.
Methods: This study reviewed the medical records of 90 adult patients with ESRD on venoarterial ECMO in intensive care units in Linkou Chang Gung Memorial Hospital between March 2009 and February 2022. Fourteen patients who died within 24 h of receiving ECMO support were excluded; the remaining 76 patients were enrolled. Demographic, clinical, and laboratory variables were retrospectively collected as survival predictors. The primary outcome was in-hospital mortality.
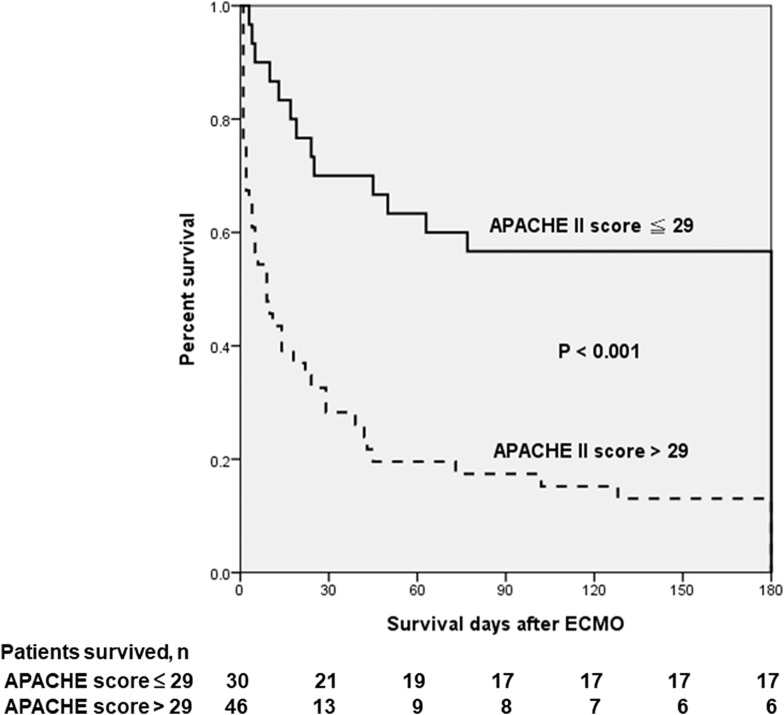
Results: The overall in-hospital mortality rate was 69.7%. The most common diagnosis requiring ECMO support was postcardiotomy cardiogenic shock, and the most frequent ECMO-associated complication was infection. Multiple logistic regression analysis revealed that the Acute Physiology and Chronic Health Evaluation II (APACHE II) score on day 1 of ECMO support was an independent risk factor for in-hospital mortality. The APACHE II score demonstrated satisfactory discriminative power (0.788 ± 0.057) in the area under the receiver operating characteristic curve. The cumulative survival rates at the 6-month follow-up differed significantly (p < 0.001) between patients with APACHE II score ≤ 29 versus those with APACHE II score >29.
Conclusion: For patients with ESRD on ECMO, the APACHE II score is an excellent predictor of in-hospital mortality.
期刊介绍:
The journal ''Cardiorenal Medicine'' explores the mechanisms by which obesity and other metabolic abnormalities promote the pathogenesis and progression of heart and kidney disease (cardiorenal metabolic syndrome). It provides an interdisciplinary platform for the advancement of research and clinical practice, focussing on translational issues.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
