Predictive models of in-hospital deterioration of Society of Cardiovascular Angiography and Intervention shock stage in patients with acute myocardial infarction initially presenting with stable hemodynamic condition.
{"title":"Predictive models of in-hospital deterioration of Society of Cardiovascular Angiography and Intervention shock stage in patients with acute myocardial infarction initially presenting with stable hemodynamic condition.","authors":"Takuto Mukaida, Yu Kataoka, Kota Murai, Kenichiro Sawada, Takamasa Iwai, Hideo Matama, Satoshi Honda, Masashi Fujino, Shuichi Yoneda, Kensuke Takagi, Kazuhiro Nakao, Fumiyuki Otsuka, Yoshio Tahara, Yasuhide Asaumi, Teruo Noguchi","doi":"10.21037/cdt-24-226","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Society of Cardiovascular Angiography and Intervention (SCAI) has defined 5 stages of cardiogenic shock (CS). In patients with acute myocardial infarction (AMI) who initially present in stable hemodynamic condition (SCAI CS stage: A or B), CS stages could deteriorate despite therapeutic management. However, deterioration of SCAI CS stages after AMI remains to be fully characterized. Therefore, the current study sought to investigate the frequency and clinical characteristics about deterioration of SCAI CS stages after AMI.</p><p><strong>Methods: </strong>We retrospectively analyzed 347 patients in a derivation cohort and 163 patients in a validation cohort who had AMI (SCAI shock stage upon arrival: A/B) and underwent percutaneous coronary intervention (PCI) at National Cerebral and Cardiovascular Center, Suita, Japan (enrolment period of study subjects: 2019.07.01-2022.09.30). Deterioration of CS (D-CS) was defined as SCAI shock stage C-E after PCI. Clinical characteristics and in-hospital mortality were compared according to D-CS status. Adjusted hazard ratios (HRs) for in-hospital mortality were calculated with multivariate Cox proportional hazards models that included variables with P<0.10 in univariate models. Uni- and multivariate logistic regression analyses were used to identify predictors of D-CS.</p><p><strong>Results: </strong>D-CS occurred in 17.3% (60/347) of the derivation cohort. Patients with D-CS had lower systolic blood pressure (BP) (P<0.001) and left ventricular ejection fraction (LVEF) (P<0.001) upon arrival with a higher proportion of initial Thrombolysis in Myocardial Infarction (TIMI) grade flow 0 or 1 (P=0.002). During hospitalization (13.9±9.4 days), D-CS was associated with higher in-hospital mortality [adjusted HR, 12.95; 95% confidence interval (CI): 1.46-114.97; P=0.02]. Initial systolic BP, LVEF, and TIMI grade flow 0 or 1 independently predicted D-CS. The D-CS risk score including these variables satisfactorily predicted D-CS [area under the curve (AUC), 0.749; 95% CI: 0.651-0.848] and in-hospital mortality (AUC, 0.961; 95% CI: 0.914-1.000) in the validation cohort.</p><p><strong>Conclusions: </strong>D-CS occurred in 17.3% of patients with AMI initially presenting in stable condition and increased the risk of in-hospital mortality. Our D-CS risk score (initial systolic BP, LVEF, and TIMI grade flow) could be helpful to predict D-CS.</p>","PeriodicalId":9592,"journal":{"name":"Cardiovascular diagnosis and therapy","volume":"14 6","pages":"1148-1160"},"PeriodicalIF":2.1000,"publicationDate":"2024-12-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11707481/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular diagnosis and therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/cdt-24-226","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/12 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The Society of Cardiovascular Angiography and Intervention (SCAI) has defined 5 stages of cardiogenic shock (CS). In patients with acute myocardial infarction (AMI) who initially present in stable hemodynamic condition (SCAI CS stage: A or B), CS stages could deteriorate despite therapeutic management. However, deterioration of SCAI CS stages after AMI remains to be fully characterized. Therefore, the current study sought to investigate the frequency and clinical characteristics about deterioration of SCAI CS stages after AMI.
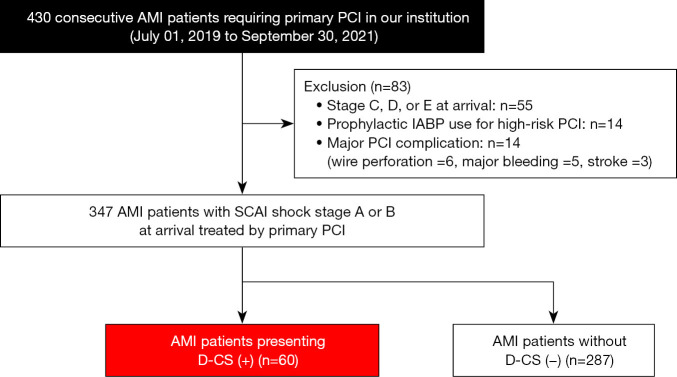
Methods: We retrospectively analyzed 347 patients in a derivation cohort and 163 patients in a validation cohort who had AMI (SCAI shock stage upon arrival: A/B) and underwent percutaneous coronary intervention (PCI) at National Cerebral and Cardiovascular Center, Suita, Japan (enrolment period of study subjects: 2019.07.01-2022.09.30). Deterioration of CS (D-CS) was defined as SCAI shock stage C-E after PCI. Clinical characteristics and in-hospital mortality were compared according to D-CS status. Adjusted hazard ratios (HRs) for in-hospital mortality were calculated with multivariate Cox proportional hazards models that included variables with P<0.10 in univariate models. Uni- and multivariate logistic regression analyses were used to identify predictors of D-CS.
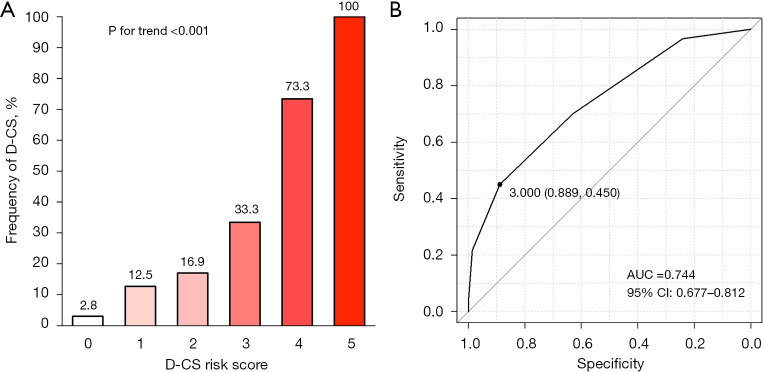
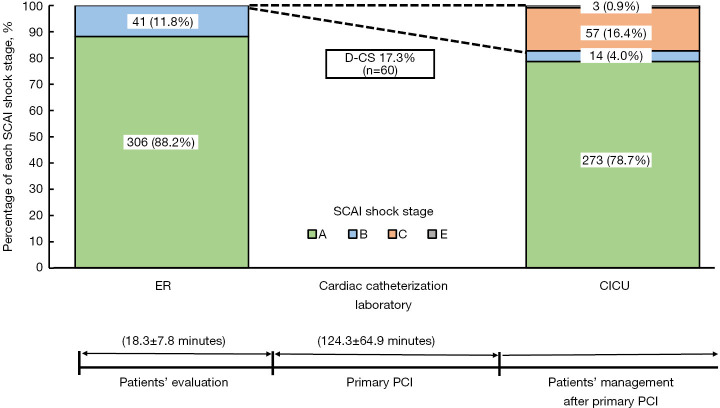
Results: D-CS occurred in 17.3% (60/347) of the derivation cohort. Patients with D-CS had lower systolic blood pressure (BP) (P<0.001) and left ventricular ejection fraction (LVEF) (P<0.001) upon arrival with a higher proportion of initial Thrombolysis in Myocardial Infarction (TIMI) grade flow 0 or 1 (P=0.002). During hospitalization (13.9±9.4 days), D-CS was associated with higher in-hospital mortality [adjusted HR, 12.95; 95% confidence interval (CI): 1.46-114.97; P=0.02]. Initial systolic BP, LVEF, and TIMI grade flow 0 or 1 independently predicted D-CS. The D-CS risk score including these variables satisfactorily predicted D-CS [area under the curve (AUC), 0.749; 95% CI: 0.651-0.848] and in-hospital mortality (AUC, 0.961; 95% CI: 0.914-1.000) in the validation cohort.
Conclusions: D-CS occurred in 17.3% of patients with AMI initially presenting in stable condition and increased the risk of in-hospital mortality. Our D-CS risk score (initial systolic BP, LVEF, and TIMI grade flow) could be helpful to predict D-CS.
期刊介绍:
The journal ''Cardiovascular Diagnosis and Therapy'' (Print ISSN: 2223-3652; Online ISSN: 2223-3660) accepts basic and clinical science submissions related to Cardiovascular Medicine and Surgery. The mission of the journal is the rapid exchange of scientific information between clinicians and scientists worldwide. To reach this goal, the journal will focus on novel media, using a web-based, digital format in addition to traditional print-version. This includes on-line submission, review, publication, and distribution. The digital format will also allow submission of extensive supporting visual material, both images and video. The website www.thecdt.org will serve as the central hub and also allow posting of comments and on-line discussion. The web-site of the journal will be linked to a number of international web-sites (e.g. www.dxy.cn), which will significantly expand the distribution of its contents.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
