Sebastian Regnery , Efthimios Katsigiannopulos , Hin Lau , Philipp Hoegen-Saßmannshausen , Fabian Weykamp , Claudia Katharina Renkamp , Carolin Rippke , Fabian Schlüter , Sophia Albert , Jan Meis , Marietta Kirchner , Alexandra Balzer , Nicolaus Andratschke , Matthias Guckenberger , Jürgen Debus , Sebastian Klüter , Juliane Hörner-Rieber
{"title":"How to protect the proximal bronchial tree during stereotactic radiotherapy of ultracentral lung tumors: Lessons from MR-guided treatment","authors":"Sebastian Regnery , Efthimios Katsigiannopulos , Hin Lau , Philipp Hoegen-Saßmannshausen , Fabian Weykamp , Claudia Katharina Renkamp , Carolin Rippke , Fabian Schlüter , Sophia Albert , Jan Meis , Marietta Kirchner , Alexandra Balzer , Nicolaus Andratschke , Matthias Guckenberger , Jürgen Debus , Sebastian Klüter , Juliane Hörner-Rieber","doi":"10.1016/j.ctro.2024.100899","DOIUrl":null,"url":null,"abstract":"<div><h3>Purpose</h3><div>To use imaging data from stereotactic MR-guided online adaptive radiotherapy (SMART) of ultracentral lung tumors (ULT) for development of a safe non-adaptive approach towards stereotactic body radiotherapy (SBRT) of ULT.</div></div><div><h3>Patients and Methods</h3><div>Analysis is based on 19 patients with ULT who received SMART (10 × 5.0–5.5 Gy) on a 0.35 T MR-Linac (MRIdian®) in the prospective MAGELLAN trial. 4D-planning CT data of six patients served to quantify proximal bronchial tree (PBT) breathing motion. Daily fraction MRIs are used to calculate interfractional translations (mediolateral (ML), anterior-posterior (AP), superior-inferior (SI)) and their dosimetric consequences for the PBT. A planning risk volume (PRV) is calculated for an assumed non-adaptive SBRT in deep-inspiration breath hold (DIBH) with surface-guidance (AlignRT®). Finally, non-adaptive volumetric modulated arc (VMAT) SBRT is simulated with and without a PRV for N = 10 patients (10 × 5.5 Gy).</div></div><div><h3>Results</h3><div>The PBT shows relevant breathing motion, especially in superior-inferior direction (median ML: 2.5 mm, AP: 1.9 mm and SI: 9.2 mm). Furthermore, moderate interfractional translations are observed (mean absolute translation ML: 1.3 mm, AP: 1.3 mm, SI: 1.1 mm), with an estimated 2 mm PRV margin for interfractional changes alone. Simulated non-adaptive SBRT leads to PBT overdoses in 60 % of patients (median overdosed fractions VMAT: 2.5, predicted MR-linac plans 4). Both MR-guided online plan adaptation (SMART) and PRV-based non-adaptive VMAT prevent PBT overdoses, but SMART yields significantly higher planning target volume (PTV) coverage (SMART: median 96 % [IQR 95–96], VMAT: median 89 % [IQR 77–94], p = 0.014).</div></div><div><h3>Conclusions</h3><div>Both intrafractional breathing motion and interfractional translations may impact doses to the PBT during SBRT of ULT. SMART protects the PBT from overdoses while maintaining high PTV coverage. Non-adaptive SBRT appears safe with advanced breathing motion management and PRV, but yields inferior PTV coverage.</div></div>","PeriodicalId":10342,"journal":{"name":"Clinical and Translational Radiation Oncology","volume":"51 ","pages":"Article 100899"},"PeriodicalIF":2.7000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11714375/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Radiation Oncology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2405630824001769","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/7 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose
To use imaging data from stereotactic MR-guided online adaptive radiotherapy (SMART) of ultracentral lung tumors (ULT) for development of a safe non-adaptive approach towards stereotactic body radiotherapy (SBRT) of ULT.
Patients and Methods
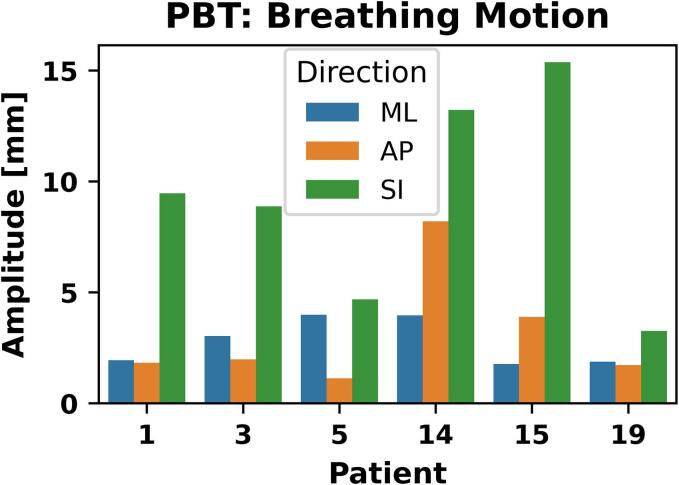
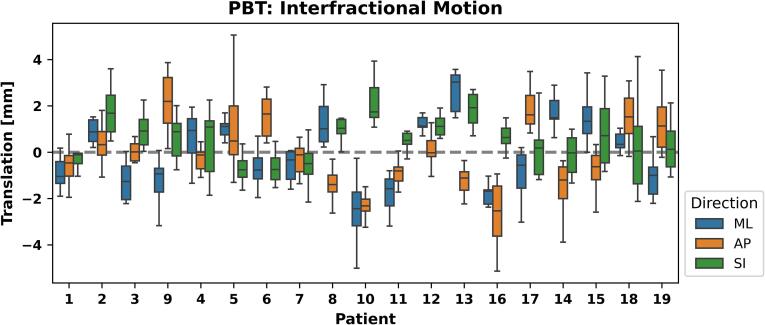
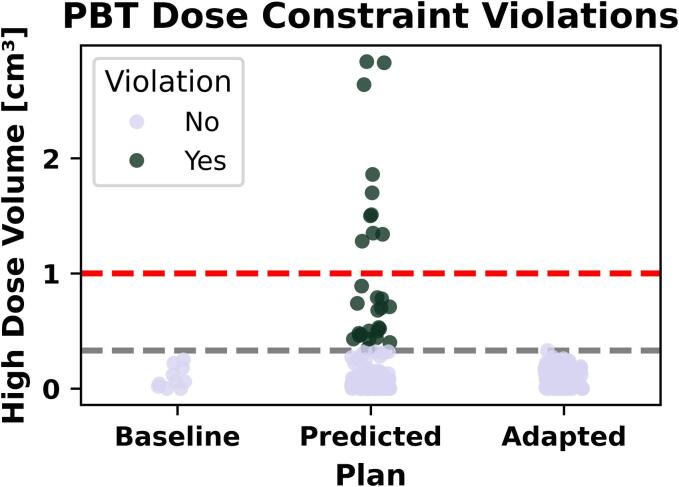
Analysis is based on 19 patients with ULT who received SMART (10 × 5.0–5.5 Gy) on a 0.35 T MR-Linac (MRIdian®) in the prospective MAGELLAN trial. 4D-planning CT data of six patients served to quantify proximal bronchial tree (PBT) breathing motion. Daily fraction MRIs are used to calculate interfractional translations (mediolateral (ML), anterior-posterior (AP), superior-inferior (SI)) and their dosimetric consequences for the PBT. A planning risk volume (PRV) is calculated for an assumed non-adaptive SBRT in deep-inspiration breath hold (DIBH) with surface-guidance (AlignRT®). Finally, non-adaptive volumetric modulated arc (VMAT) SBRT is simulated with and without a PRV for N = 10 patients (10 × 5.5 Gy).
Results
The PBT shows relevant breathing motion, especially in superior-inferior direction (median ML: 2.5 mm, AP: 1.9 mm and SI: 9.2 mm). Furthermore, moderate interfractional translations are observed (mean absolute translation ML: 1.3 mm, AP: 1.3 mm, SI: 1.1 mm), with an estimated 2 mm PRV margin for interfractional changes alone. Simulated non-adaptive SBRT leads to PBT overdoses in 60 % of patients (median overdosed fractions VMAT: 2.5, predicted MR-linac plans 4). Both MR-guided online plan adaptation (SMART) and PRV-based non-adaptive VMAT prevent PBT overdoses, but SMART yields significantly higher planning target volume (PTV) coverage (SMART: median 96 % [IQR 95–96], VMAT: median 89 % [IQR 77–94], p = 0.014).
Conclusions
Both intrafractional breathing motion and interfractional translations may impact doses to the PBT during SBRT of ULT. SMART protects the PBT from overdoses while maintaining high PTV coverage. Non-adaptive SBRT appears safe with advanced breathing motion management and PRV, but yields inferior PTV coverage.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
