{"title":"Real-world cost-effectiveness analysis of thymoglobulin versus no induction therapy in kidney transplant recipients at low risk of graft loss.","authors":"Adrieli Barros Bessa, Marina Pontello Cristelli, Claudia Rosso Felipe, Renato Demarchi Foresto, Marcelo Cunio Machado Fonseca, Jose Medina Pestana, Helio Tedesco-Silva","doi":"10.1590/2175-8239-JBN-2024-0060en","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A new induction therapy strategy of a single 3 mg/kg dose of rabbit antithymocyte globulin (r-ATG) showed a lower incidence of acute rejection.</p><p><strong>Methods: </strong>The objective of this study was to use real-world data to determine the incremental cost-effectiveness ratio (ICER) of r-ATG induction for the prevention of acute rejection (AR) in the first year following kidney transplantation and for kidney graft survival over 1, 4, and 10 years of post-transplantation from the perspective of the national public healthcare system. A Markov state transition model was developed utilizing real-world data extracted from medical invoices from a single center. The study population consisted of adults at low immunological risk undergoing their initial transplantation and received kidneys from either living or deceased donors. The intervention of r-ATG induction was compared to no induction. The clinical outcomes considered for this analysis were acute rejection, cytomegalovirus infection/disease, death, graft loss, and retransplantation.</p><p><strong>Results: </strong>The cost-effectiveness analysis in the first year revealed that the r-ATG group was more cost-effective, with an ICER of US$ 399.96 per avoided AR episode, an effectiveness gain of 0.01 year in graft survival and a total incremental cost of US$ 147.50. The 4- and 10-year analyses revealed an effectiveness gain of 0.06 and 0.16 years in graft survival in the r-ATG induction group, and a total incremental cost of US$ -321.68 and US$ -2,440.62, respectively.</p><p><strong>Conclusion: </strong>The single 3 mg/kg dose of r-ATG is cost-effective in preventing acute rejection episodes and dominant in the long term of transplantation, conferring survival gain.</p>","PeriodicalId":14724,"journal":{"name":"Jornal brasileiro de nefrologia : 'orgao oficial de Sociedades Brasileira e Latino-Americana de Nefrologia","volume":"47 1","pages":"e20240060"},"PeriodicalIF":1.3000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11772011/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Jornal brasileiro de nefrologia : 'orgao oficial de Sociedades Brasileira e Latino-Americana de Nefrologia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1590/2175-8239-JBN-2024-0060en","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A new induction therapy strategy of a single 3 mg/kg dose of rabbit antithymocyte globulin (r-ATG) showed a lower incidence of acute rejection.
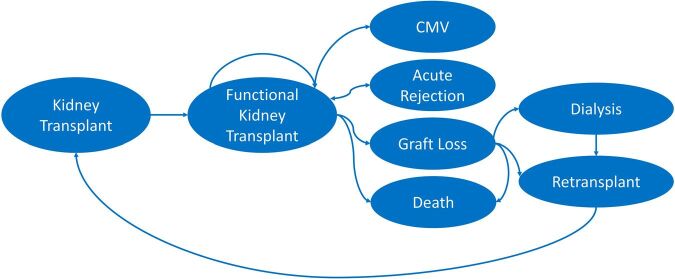
Methods: The objective of this study was to use real-world data to determine the incremental cost-effectiveness ratio (ICER) of r-ATG induction for the prevention of acute rejection (AR) in the first year following kidney transplantation and for kidney graft survival over 1, 4, and 10 years of post-transplantation from the perspective of the national public healthcare system. A Markov state transition model was developed utilizing real-world data extracted from medical invoices from a single center. The study population consisted of adults at low immunological risk undergoing their initial transplantation and received kidneys from either living or deceased donors. The intervention of r-ATG induction was compared to no induction. The clinical outcomes considered for this analysis were acute rejection, cytomegalovirus infection/disease, death, graft loss, and retransplantation.
Results: The cost-effectiveness analysis in the first year revealed that the r-ATG group was more cost-effective, with an ICER of US$ 399.96 per avoided AR episode, an effectiveness gain of 0.01 year in graft survival and a total incremental cost of US$ 147.50. The 4- and 10-year analyses revealed an effectiveness gain of 0.06 and 0.16 years in graft survival in the r-ATG induction group, and a total incremental cost of US$ -321.68 and US$ -2,440.62, respectively.
Conclusion: The single 3 mg/kg dose of r-ATG is cost-effective in preventing acute rejection episodes and dominant in the long term of transplantation, conferring survival gain.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
