A new insight into the anatomical ablation approach at R-L ILT for VAs with a left ventricular summit origination: electrophysiological characteristics and catheter ablation.
Yang Pang, Ye Xu, Kuan Cheng, Chaofeng Chen, Qingxing Chen, Yunlong Ling, Guijian Liu, Junbo Ge, Wenqing Zhu
{"title":"A new insight into the anatomical ablation approach at R-L ILT for VAs with a left ventricular summit origination: electrophysiological characteristics and catheter ablation.","authors":"Yang Pang, Ye Xu, Kuan Cheng, Chaofeng Chen, Qingxing Chen, Yunlong Ling, Guijian Liu, Junbo Ge, Wenqing Zhu","doi":"10.1007/s10840-024-01974-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ventricular arrhythmia (VA) originating from the left ventricular summit (LVS) poses particular challenges, with higher rates of ablation failure.</p><p><strong>Objective: </strong>To further evaluate the anatomical ablation approach from the subaortic region for LVS VAs and their electrophysiological characteristics.</p><p><strong>Method: </strong>The study enrolled 27 consecutive patients with sympatomatic VAs originating from LVS and who received an anatomical ablation approach from R-L ILT in our center.</p><p><strong>Results: </strong>Three different mapping results were obtained as the earliest activation sites (EAS) were observed in the RVOT region (group 1), R-L ILT (group 2), and epicardial region (group 3), respectively. A higher percentage of rS/QS patterns in lead I was observed in Groups 1 and 3. A narrower QRS duration was observed in Group (1) A presystolic potential was recorded at R-L ILT for most VAs in group (2) All VAs were successfully ablated at R-L ILT in groups 1 and 2, though poor pace mapping results were observed at R-L ILT. 4/7 VAs in group 3 ultimately failed after an ablation in both the endocardial and epicardial regions.</p><p><strong>Conclusion: </strong>An anatomical ablation approach at R-L ILT was effective for most VAs with an LVS origin. Different ECG and electrophysiological characteristics could be observed in VAs with different EAS. Poor pace mapping results in all regions with an EAS in the epicardial region had predictive value for the failure of the ablation procedure.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"709-720"},"PeriodicalIF":2.6000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12167298/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-024-01974-w","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/8 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Ventricular arrhythmia (VA) originating from the left ventricular summit (LVS) poses particular challenges, with higher rates of ablation failure.
Objective: To further evaluate the anatomical ablation approach from the subaortic region for LVS VAs and their electrophysiological characteristics.
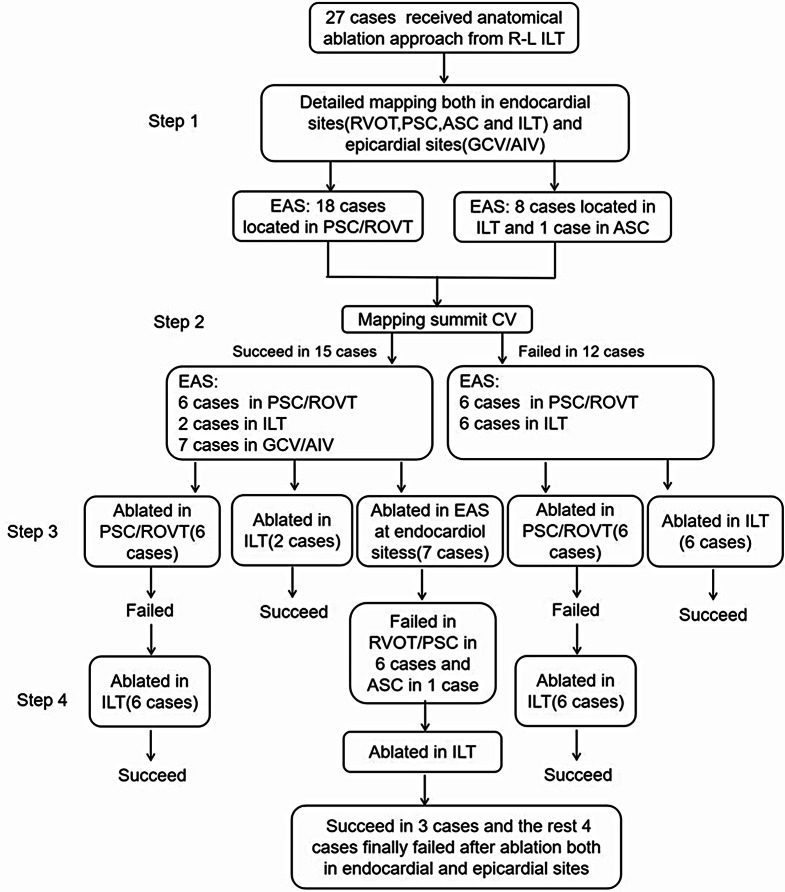
Method: The study enrolled 27 consecutive patients with sympatomatic VAs originating from LVS and who received an anatomical ablation approach from R-L ILT in our center.
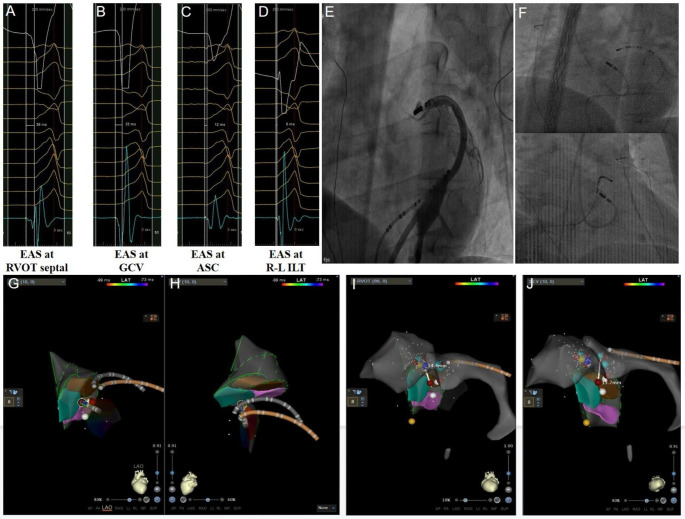
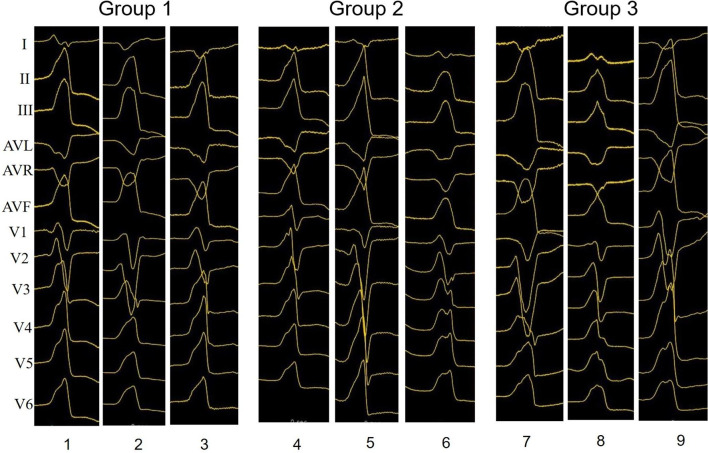
Results: Three different mapping results were obtained as the earliest activation sites (EAS) were observed in the RVOT region (group 1), R-L ILT (group 2), and epicardial region (group 3), respectively. A higher percentage of rS/QS patterns in lead I was observed in Groups 1 and 3. A narrower QRS duration was observed in Group (1) A presystolic potential was recorded at R-L ILT for most VAs in group (2) All VAs were successfully ablated at R-L ILT in groups 1 and 2, though poor pace mapping results were observed at R-L ILT. 4/7 VAs in group 3 ultimately failed after an ablation in both the endocardial and epicardial regions.
Conclusion: An anatomical ablation approach at R-L ILT was effective for most VAs with an LVS origin. Different ECG and electrophysiological characteristics could be observed in VAs with different EAS. Poor pace mapping results in all regions with an EAS in the epicardial region had predictive value for the failure of the ablation procedure.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
